OsseoSure Clinical Masterclass
The Spatiotemporal Gradient
How Bone Responds to Space, Time, and Force
29 slides · Speaker: Dr. Kedar Bakshi
Slide Gallery

Slide 1
Namaste. I am Dr. Kedar Bakshi. I have been practicing implantology for the last twenty-six years. I am the innovator of OsseoSure — a mechanical periotome and mechanical osteotome system.
Today I want to share something with you that changed the way I think about every procedure I do — not just implantology, but everything. Two words. Spatial. Temporal. Space and time.
By the end of this presentation, you will never look at a CBCT the same way again.
Slide 3
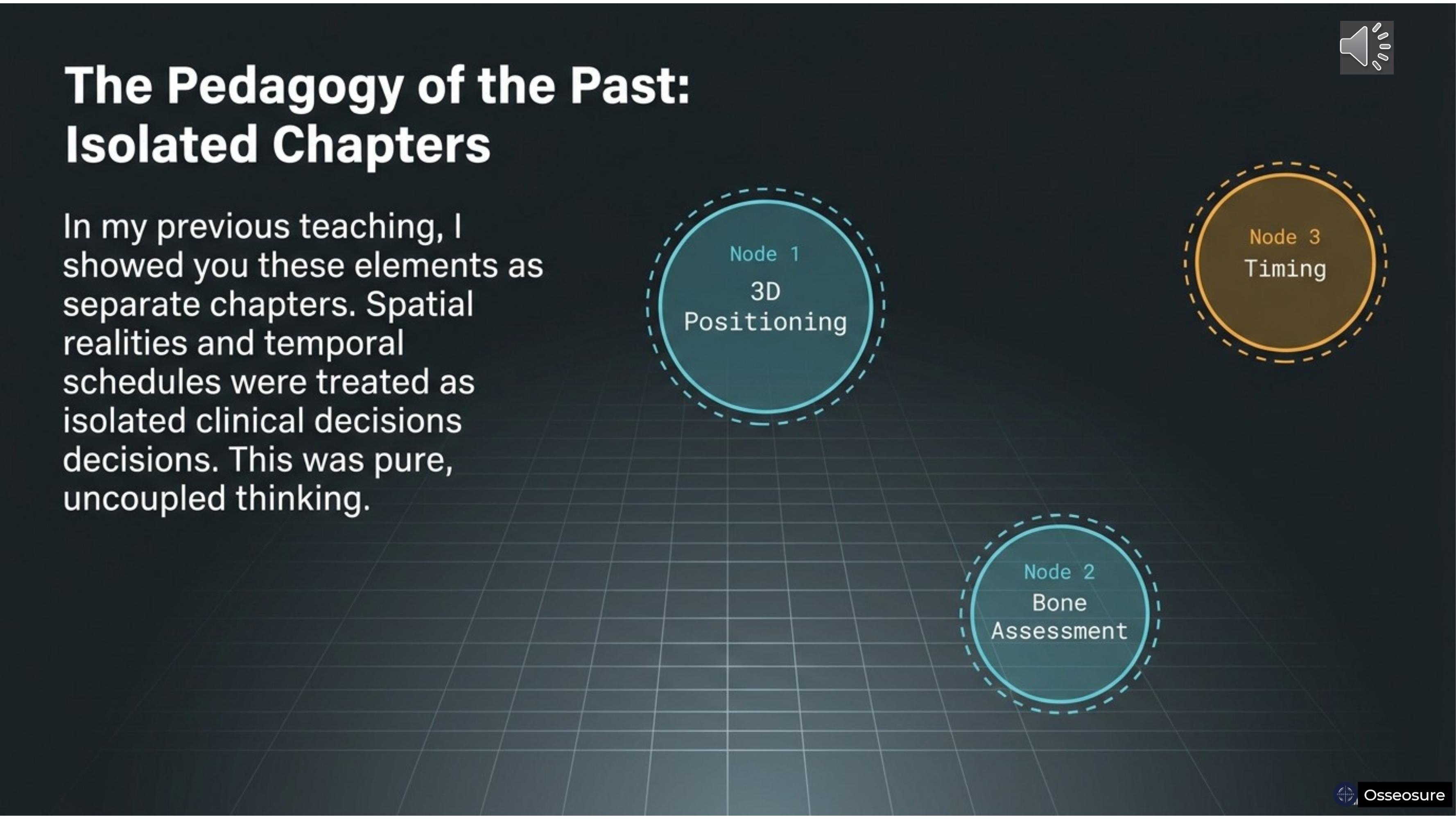
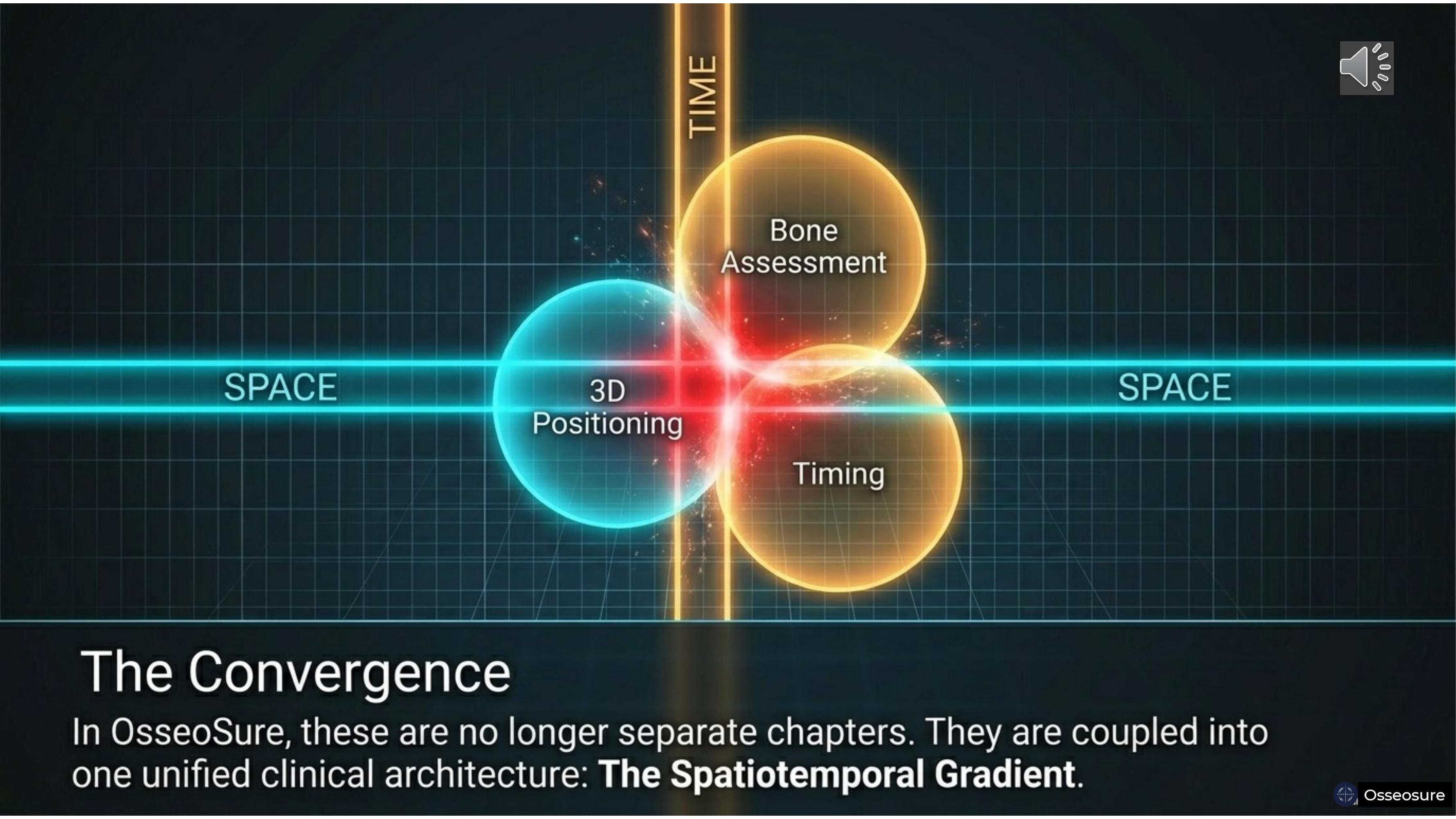
In my previous teaching, I showed you these elements as separate chapters. 3D implant positioning was one chapter. Bone assessment was another. Timing of placement and loading was a third.
You learned each one independently. Spatial realities and temporal schedules were treated as isolated clinical decisions. This was pure, uncoupled thinking.
Today I am going to show you that these were never separate. They were always connected — and OsseoSure is the instrument that couples them.
Slide 4
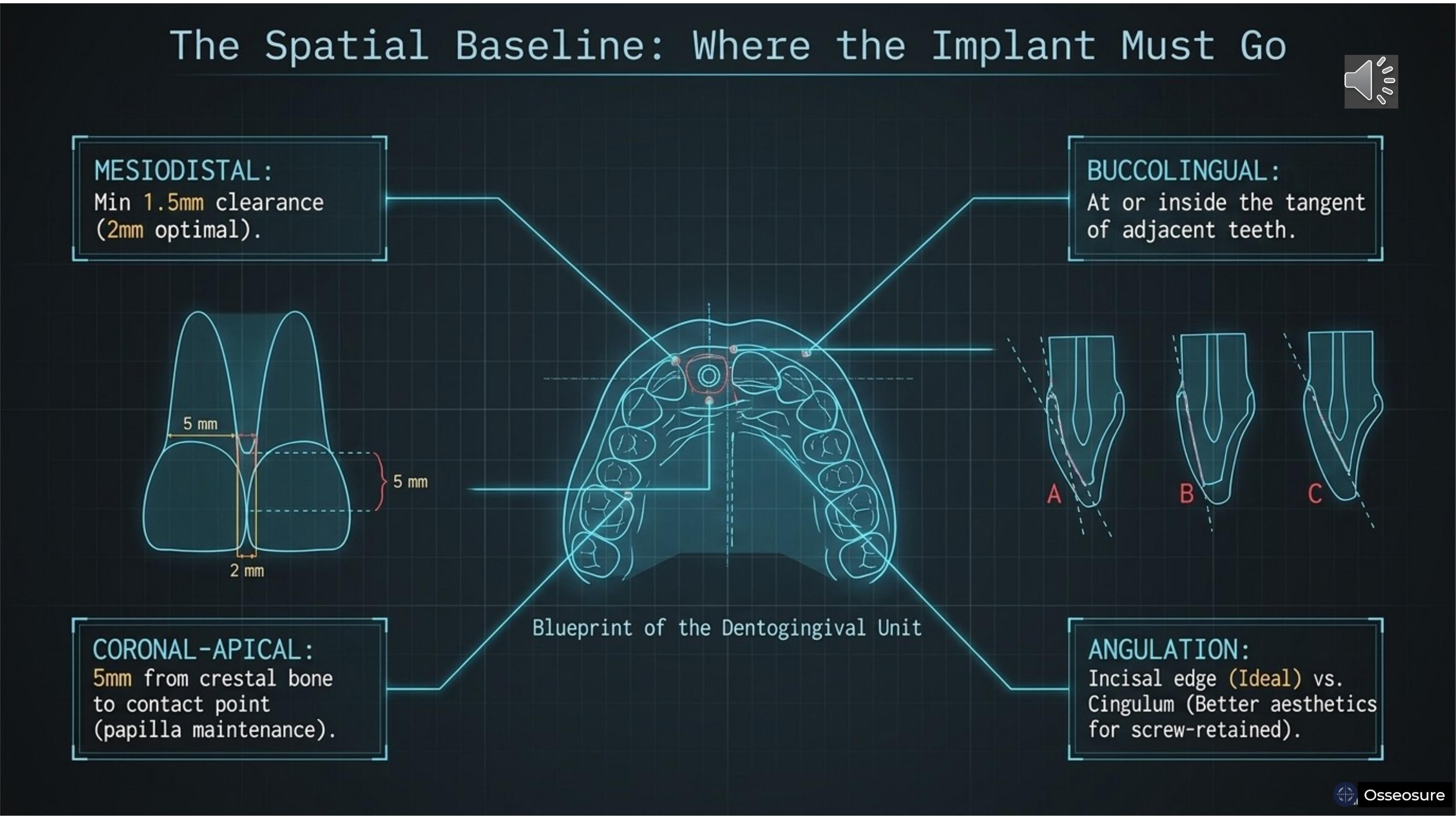
Let us start with what you already know. 3D implant positioning — three dimensions that every implant must satisfy.
Mesiodistal: minimum 1.5 millimeters clearance from adjacent teeth, with 2 millimeters being optimal. This maintains the crestal bone. contact point to crest at 5 millimeters, which is necessary for predictable interdental papilla.
Buccolingual: the implant should be placed at the tangent or inside the tangent of the arch drawn from neighbouring teeth.
Coronal-apical: correct depth for prosthetic emergence and crestal bone preservation.
And angulation — this is critical for aesthetics. Position A is the incisal edge position, considered ideal. Position B is buccal, where the tooth will look taller — not aesthetic. Position C is the cingulum position, especially for screw-retained prostheses.
A is considered better for aesthetics, These three dimensions plus angulation define WHERE the implant must go. This is pure spatial thinking. And here is an important point — you can always correct angulation with mechanical or manual osteotomes. Drilling alone will never allow you to correct angulation the way an osteotome can.
Slide 5
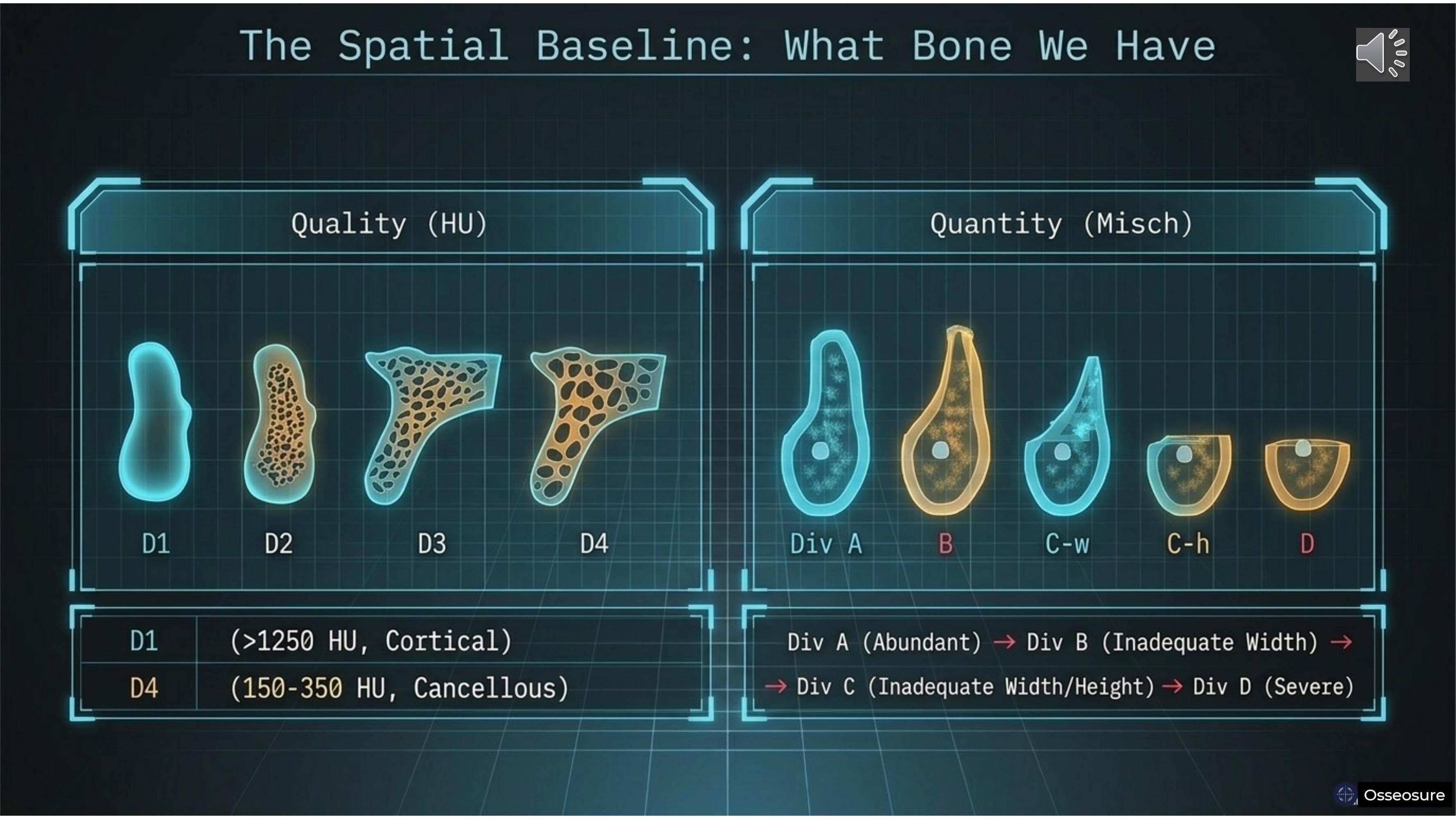
For pre-implant planning, we evaluate the available bone in two ways.
Quality: D1, D2, D3, D4 — from hard cortical at more than 1250 Hounsfield units to soft cancellous bone at 150 to 350 Hounsfield units.
Quantity: the Misch classification — Division A with abundant bone, Division B with inadequate width, Division C-W with inadequate width, Division C-H with inadequate height, and Division D with severe deficiency.
Quality tells you how the bone will respond to your instruments. Quantity tells you what bone is available to work with. Both are spatial information — they tell you what you HAVE right now.
Slide 6
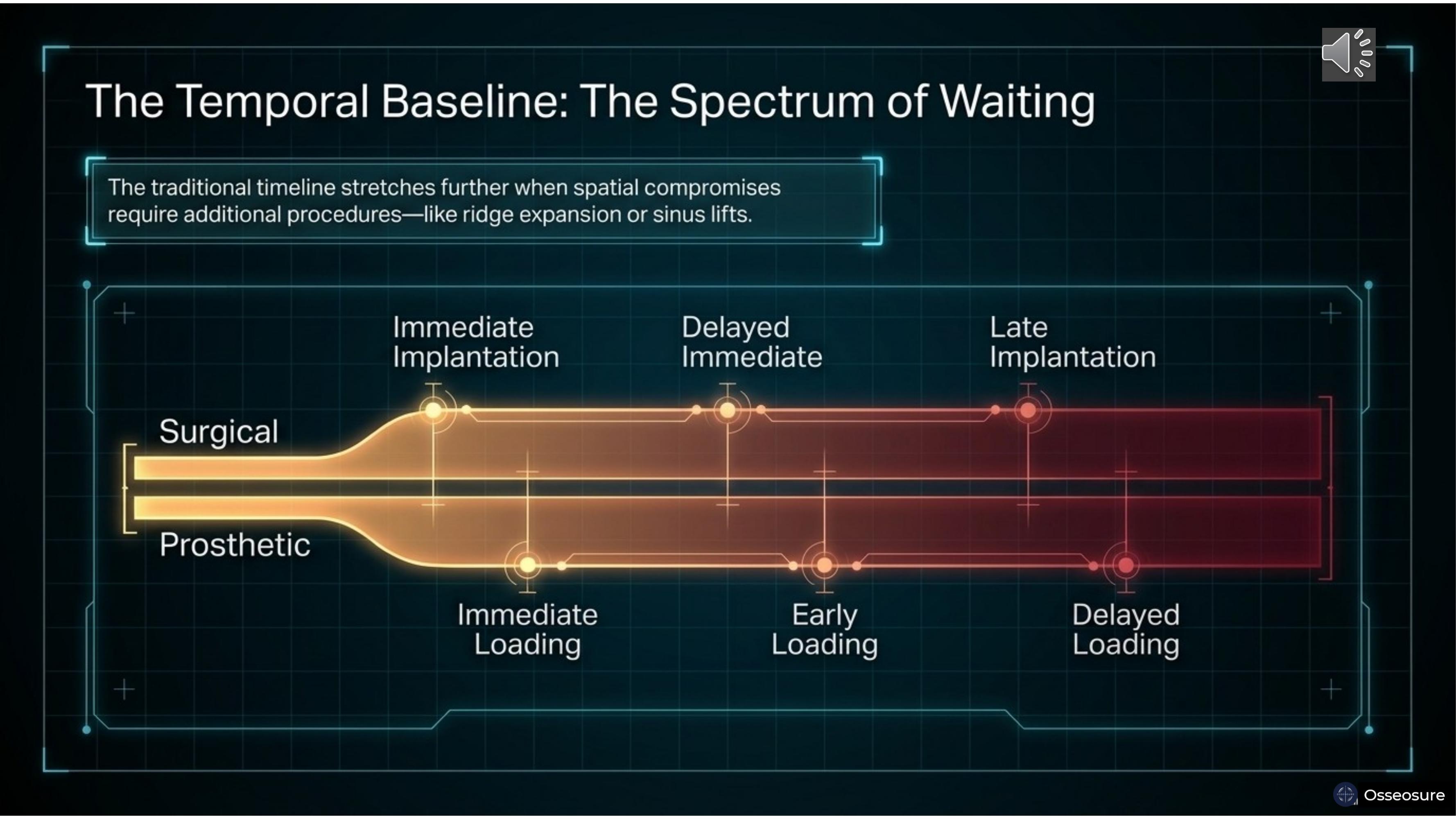
Now the temporal dimension. For placement, we have three options: immediate implantation, delayed immediate implantation, and late implantation.
For loading, we also have three options: immediate loading, early loading, and conventional loading — which is also called delayed loading. In conventional loading, we wait approximately four months. In delayed loading, we may add an additional one to two months for progressive bone loading — allowing the bone to gradually adapt to functional forces before full prosthetic loading.
This gives you a spectrum — from the fastest pathway, immediate implantation with immediate loading, to the most delayed, late implantation with conventional or delayed loading. And if any additional procedure is needed like sinus lift — the temporal timeline extends further.
This is pure temporal thinking. When do I place? When do I load?
Slide 7
Now here is what I want to share with you today.
3D implant positioning. Bone quality. Bone quantity. Timing of placement. Timing of loading. These were always taught as separate chapters.
But in OsseoSure, I have coupled all of them into one unified framework.
The quality and quantity of bone — D1 through D4, Division A through D — are coupled into the Four-Quadrant Decision Matrix: narrow-hard, narrow-soft, wide-hard, wide-soft. That is the spatial component.
The timing of placement and loading — immediate, delayed immediate, or late, combined with immediate, early, or conventional loading — is the temporal component.
And 3D implant positioning — placing the implant at the incisal edge or cingulum position, correcting angulation with osteotomes not drills — is where space and time meet.
In mechanics, this coupling of space and time is called a spatiotemporal gradient. And that is exactly what OsseoSure delivers.
---
Slide 8
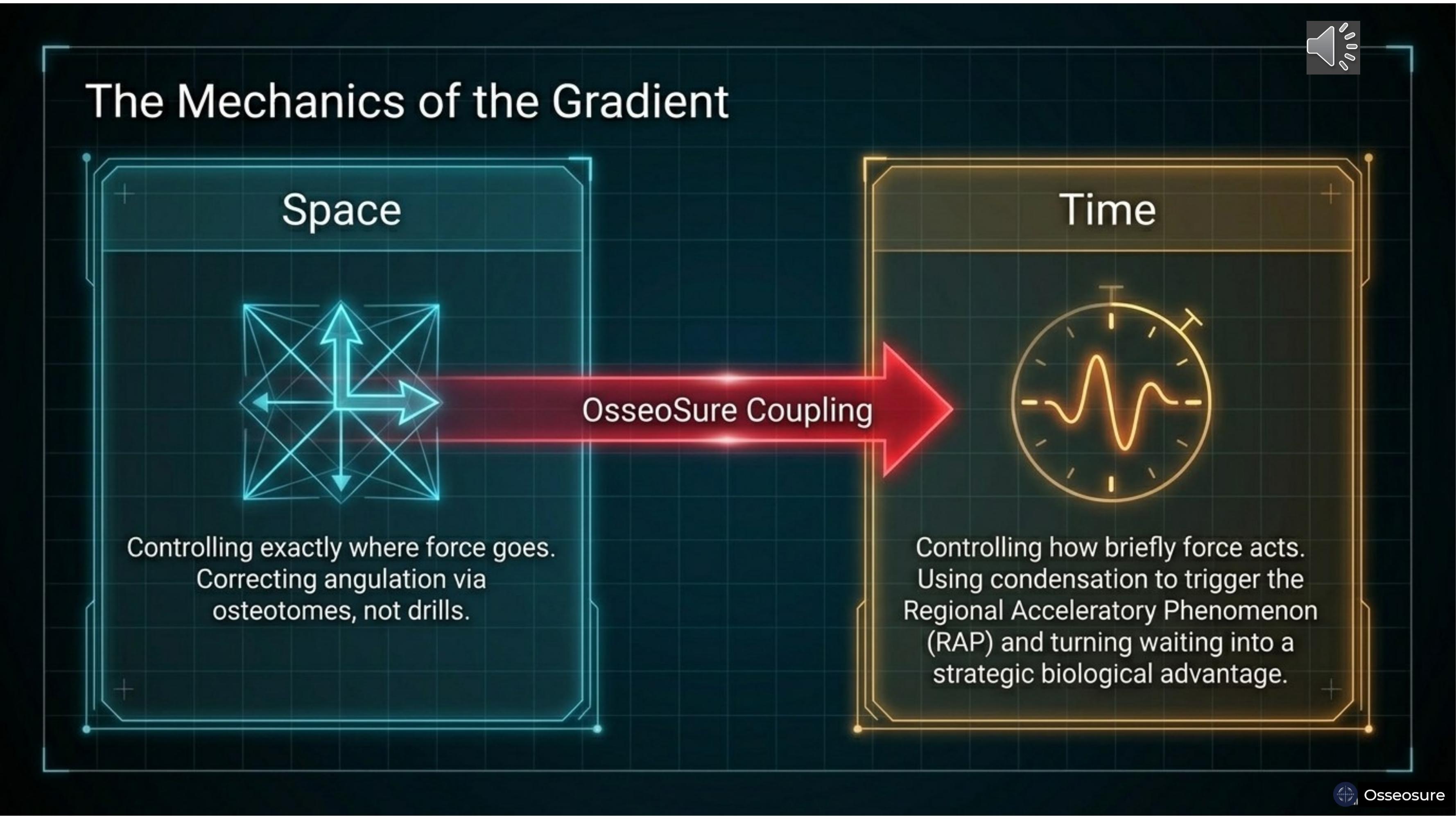
The spatial gradient controls exactly where force goes. The tapered geometry directs force precisely — and corrects angulation without drilling.
The temporal gradient controls how briefly force acts. The piston-driven mechanism delivers millisecond-duration impacts that trigger the Regional Acceleratory Phenomenon — RAP — without causing thermal necrosis.
OsseoSure couples these two. In late implantation cases, condensation and ridge split uses the spatial advantage to counteract what was lost in the temporal dimension — recovering bone width and simultaneously triggering accelerated healing. Waiting is no longer a penalty. It becomes a strategic biological advantage.
Slide 9
Let me now explain the science behind this coupling.
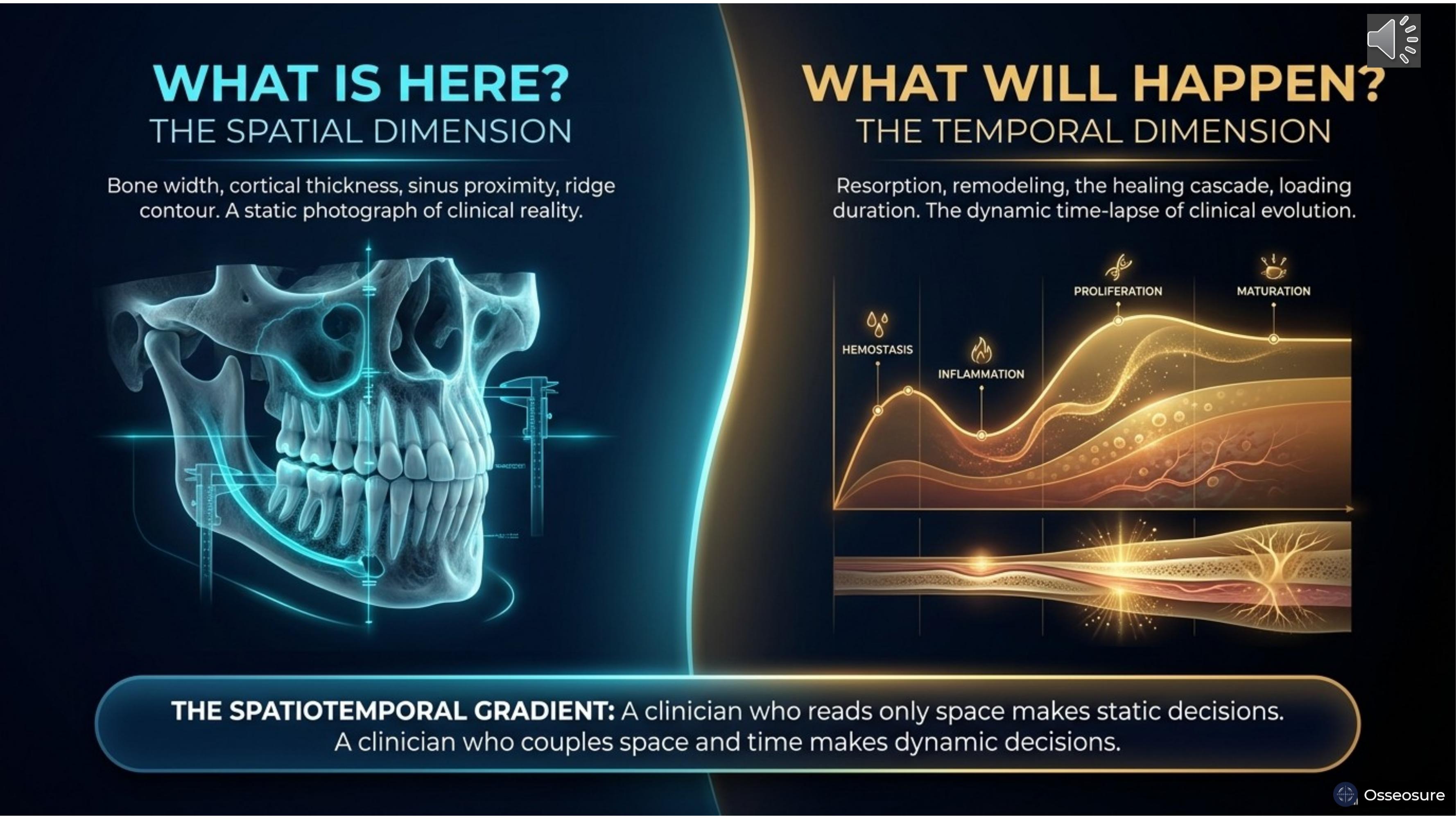
When you take a CBCT, what are you reading? You are reading space. Bone width, height, density, sinus proximity, nerve position, ridge contour. All spatial information — what exists right now, frozen in space. Spatial is the photograph.
The moment you make a clinical decision based on that CBCT, you enter the temporal dimension. If I extract this tooth, how will the ridge change over three months? If I place this implant today, how will the bone-implant interface remodel over six months? Temporal is the time-lapse video.
A clinician who reads only space makes static decisions. A clinician who couples space and time makes dynamic decisions. And dynamic decisions produce better outcomes.
Slide 10
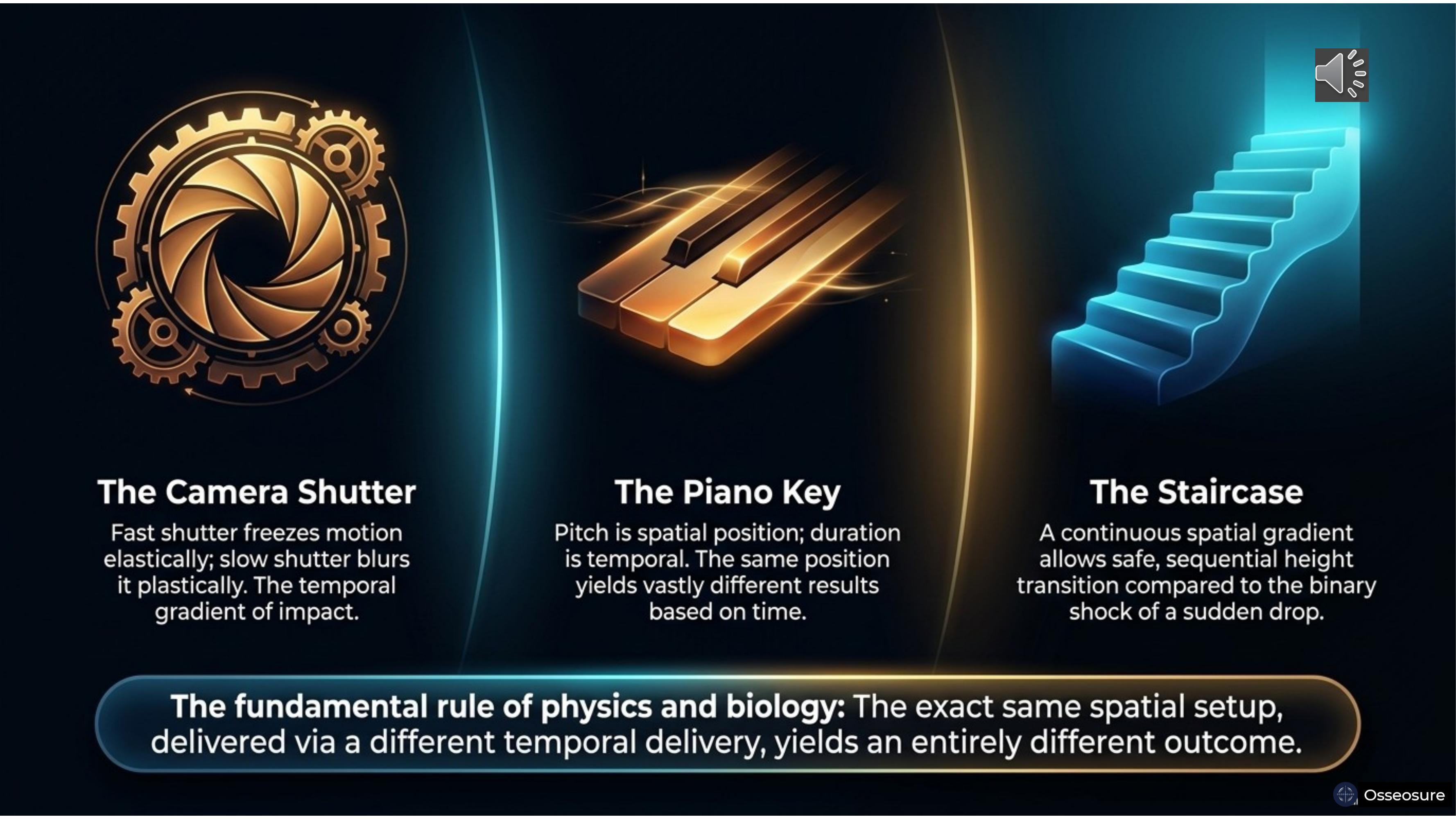
Let me make this intuitive with three analogies.
The camera shutter. A fast shutter freezes motion say.. elastically — the image is sharp. A slow shutter.. blurs it — plastic deformation. Same scene, different temporal delivery, completely different result. Bone behaves .. identically.
The piano key. Pitch is spatial — which key you press……… Duration is temporal — how long you hold it. Same note, different duration, entirely different musical experience. OsseoSure's tapered geometry controls where force goes — the spatial gradient. The piston-driven mechanism controls how briefly force acts — the temporal gradient.
The staircase. A continuous spatial gradient allows safe, sequential transition — compared to the binary shock of a sudden drop. A tapered osteotome is a staircase. A parallel osteotome is stepping off a cliff.
The fundamental rule: the exact same spatial setup, delivered via a different temporal delivery, yields an entirely different outcome.
Slide 11
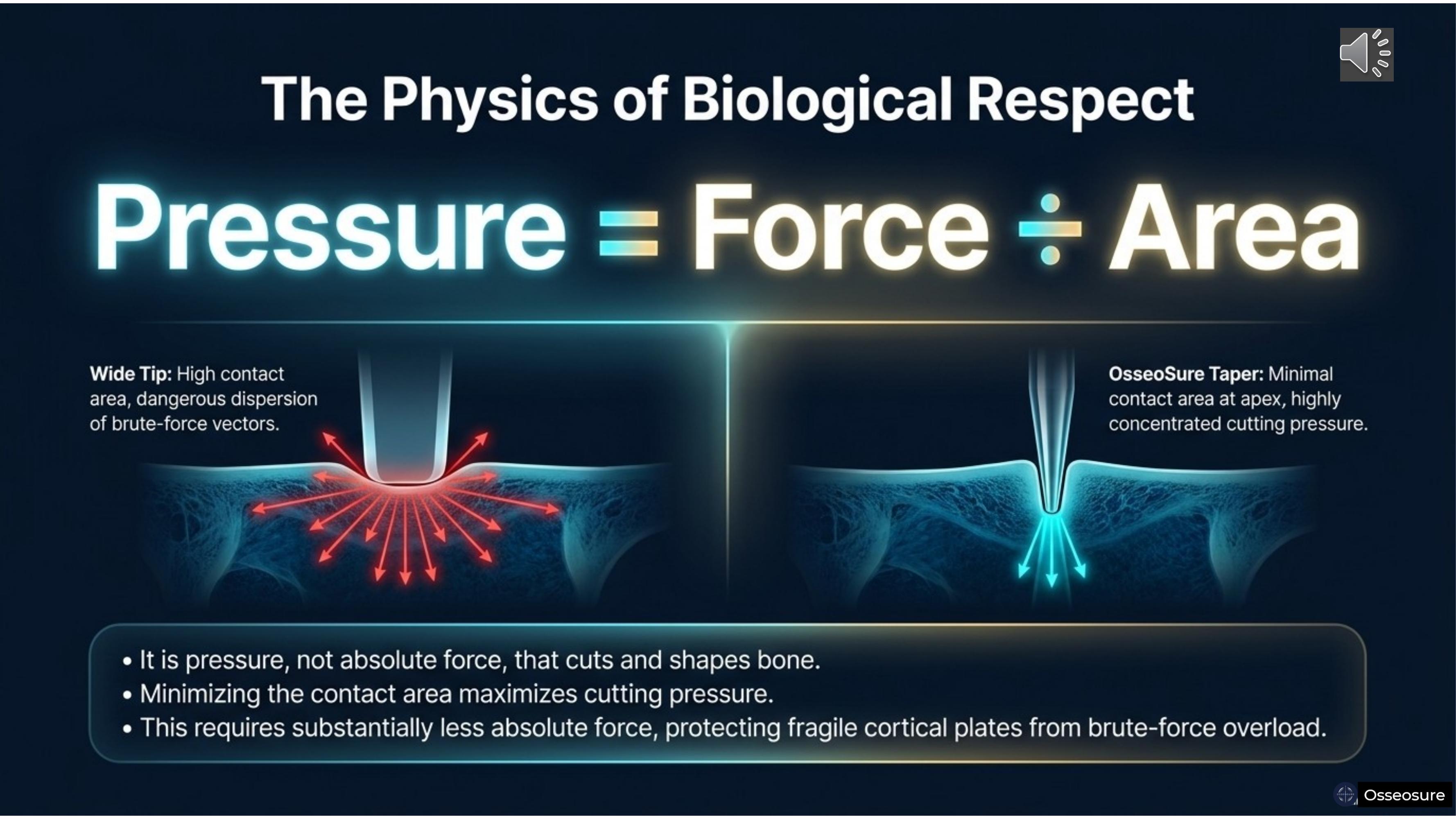
Pressure equal to force divided by area. It is pressure — not absolute force — that cuts and shapes bone.
A wide tip has a high contact area. Force disperses in all directions — brute-force vectors that damage cortical plates.
OsseoSure's tapered tip has minimal contact area at the apex. The same force is concentrated into a tiny point — highly focused cutting pressure. You need substantially less absolute force. The cortical plates are protected because the force is never brute — it is precise.
This is why OsseoSure requires less effort from the surgeon and produces less trauma to the bone.
Slide 12
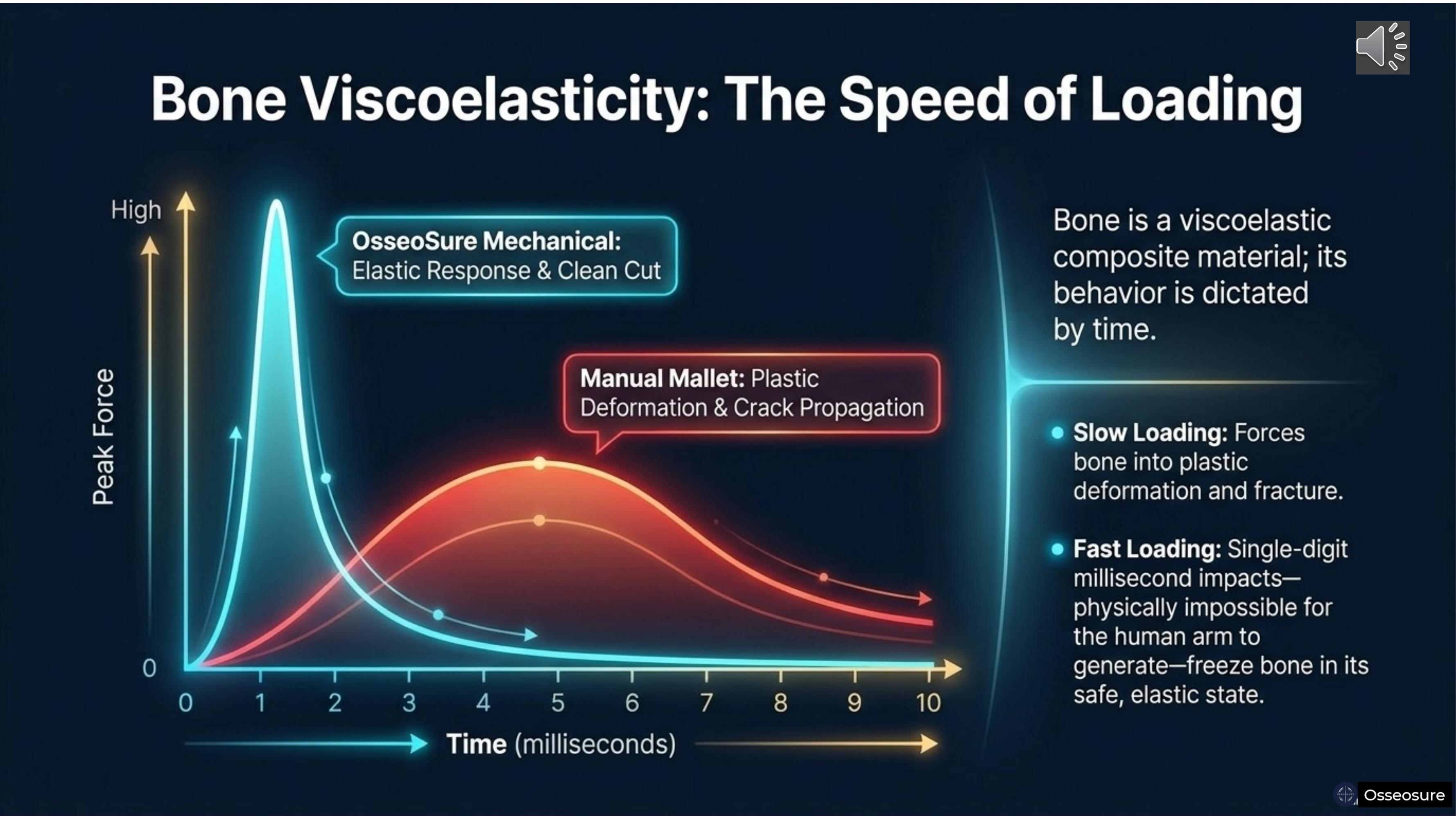
Bone is a viscoelastic composite material. Its behaviour is dictated by time.
Slow loading — forces applied over four to ten milliseconds — pushes bone into plastic deformation. Cracks propagate. Architecture is permanently damaged.
Fast loading — single-digit millisecond impacts from the piston-driven mechanism — freezes bone in its safe, elastic state. The cut is clean, the architecture recovers.
The piston delivers what the human arm physically cannot — a millisecond-duration impact that keeps bone in its elastic window. This is not a theoretical difference. This is the difference between a clean osteotomy wall that heals rapidly and a damaged wall that heals through slow creeping substitution.
Slide 13
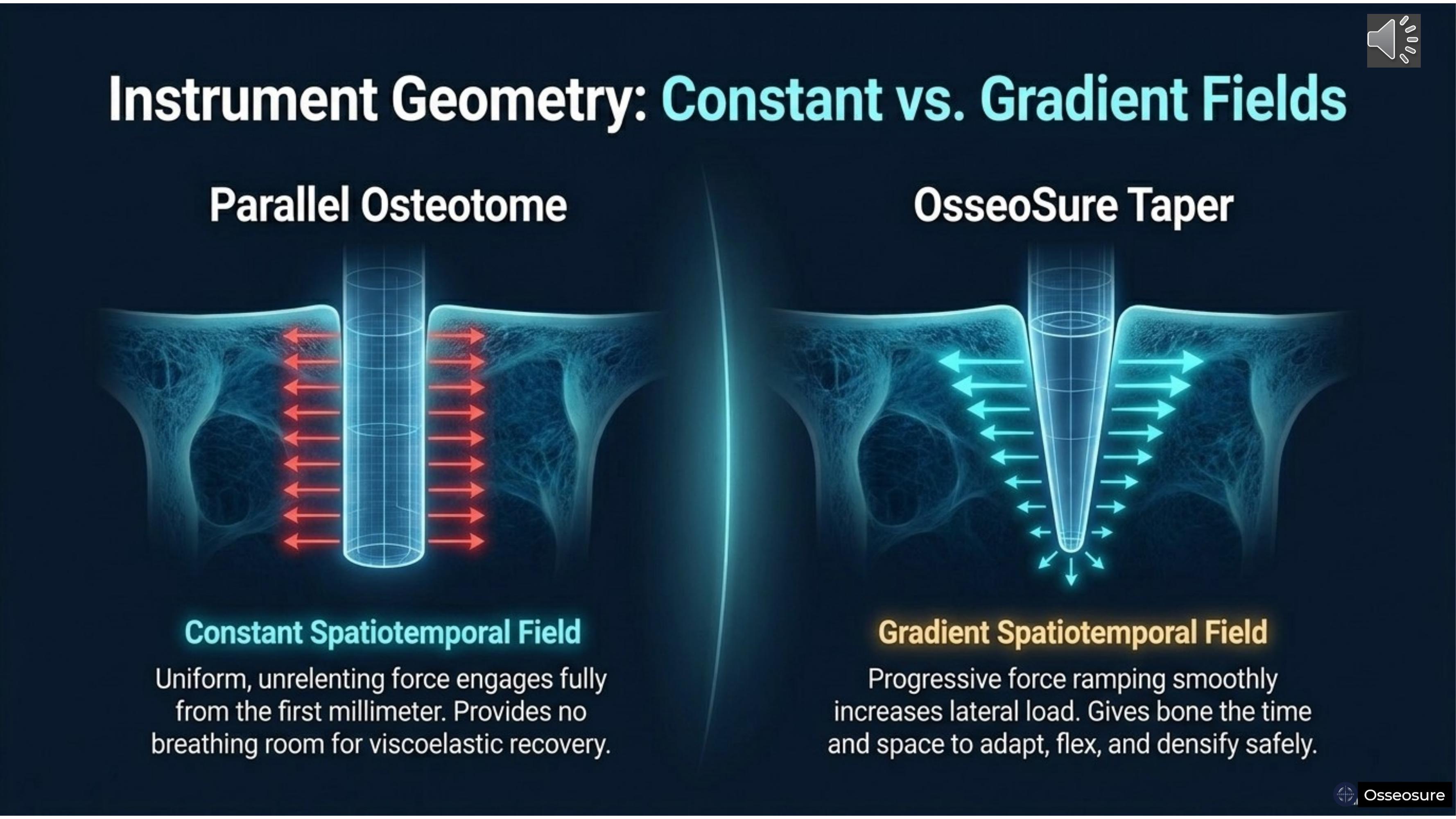
On the left — the parallel osteotome creates a constant spatiotemporal field. Uniform, unrelenting force from the first millimeter. No breathing room for viscoelastic recovery.
On the right — the OsseoSure taper creates a gradient spatiotemporal field. The narrow apex engages first — small area, minimal force. As the instrument advances deeper, wider shoulders engage progressively. Different parts of the bone are engaged at different times, in different amounts, in a smooth, continuous sequence.
The bone gets time and space to adapt, flex, and densify safely. This is the spatiotemporal gradient in clinical reality.
Slide 14
I have named two concepts from my clinical observation.
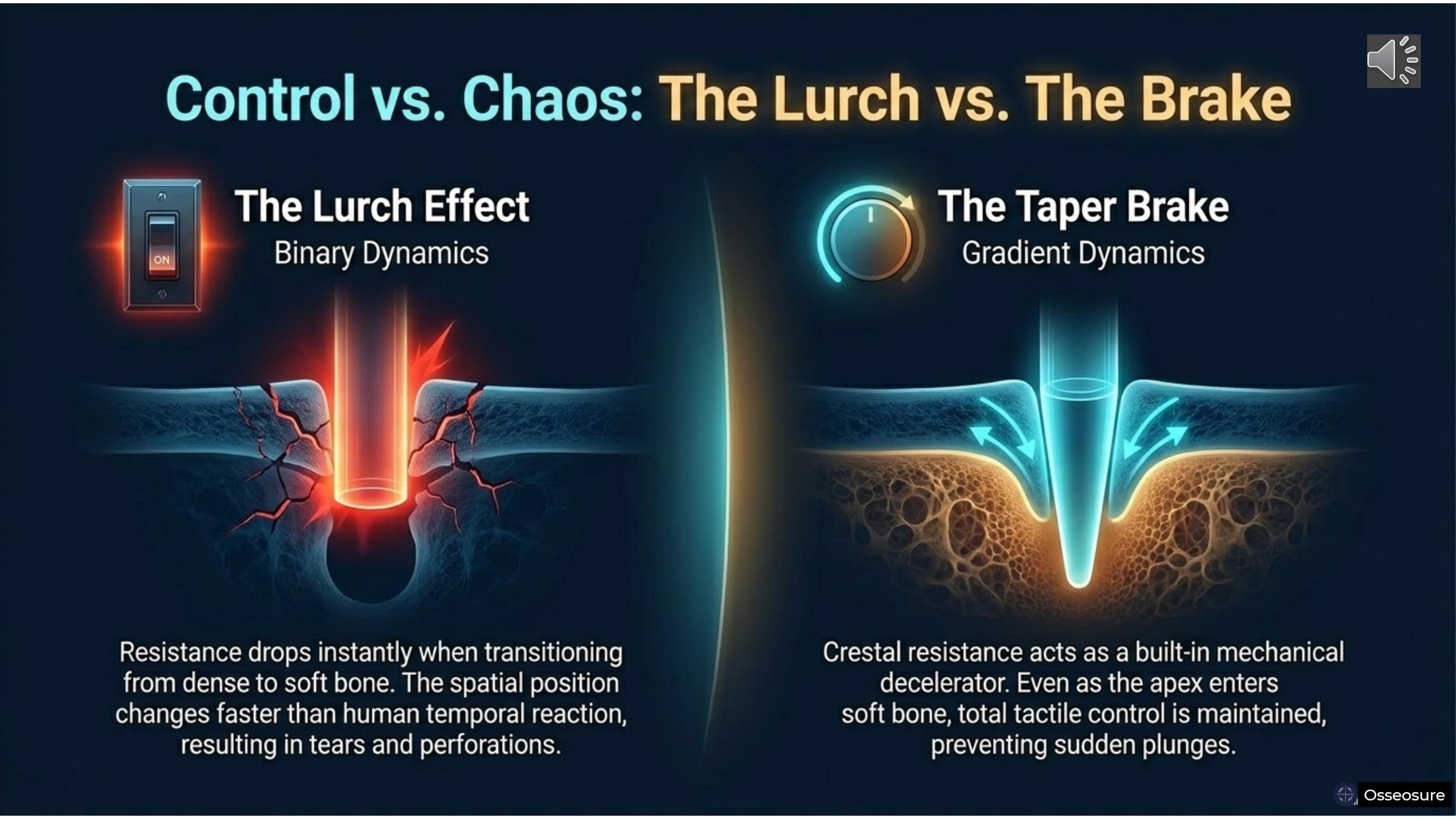
The Lurch Effect. When a parallel osteotome passes through a sudden density change — cortical bone into cancellous, or parallel ostetome breaks sinus floor. — resistance drops instantly. But the surgeon's hand is still applying the same force. The instrument lurches forward, uncontrolled. This is the biomechanical moment when sinus perforations happen.
The Taper Brake. OsseoSure's tapered geometry prevents this naturally. When the narrow apex enters softer bone, the wider crestal portion is still engaging harder bone above it. The instrument cannot lurch because crestal resistance acts as a built-in decelerator. The surgeon feels a smooth transition. There is always time to sense, respond, and stop.
Lurch Effect — the danger of parallel osteotomes. Taper Brake — the safety of taper. osteotomes
Slide 15
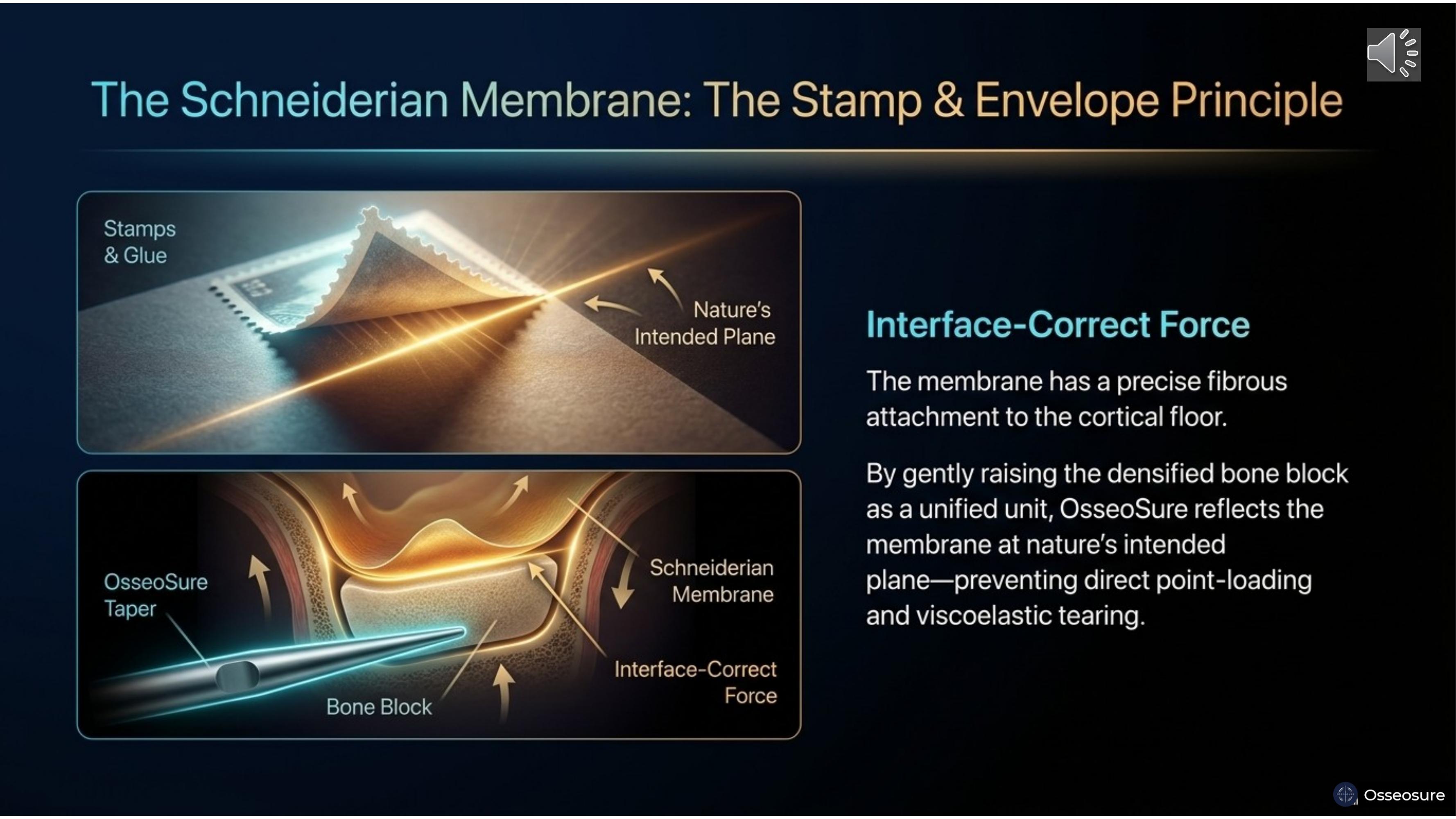
Think of a postage stamp glued to an envelope. The stamp is the Schneiderian membrane. The envelope is the cortical sinus floor. The glue is the elastic attachment.
If you poke a sharp point through the envelope, you tear the stamp. But if you gently lift the envelope itself as a unified block, the stamp lifts cleanly at nature's intended plane.
This is what OsseoSure does. The tapered osteotome condenses the bone beneath the sinus floor into a densified block. When raised gently, the Schneiderian membrane lifts with it — no direct point-loading, no tearing.
Slide 16
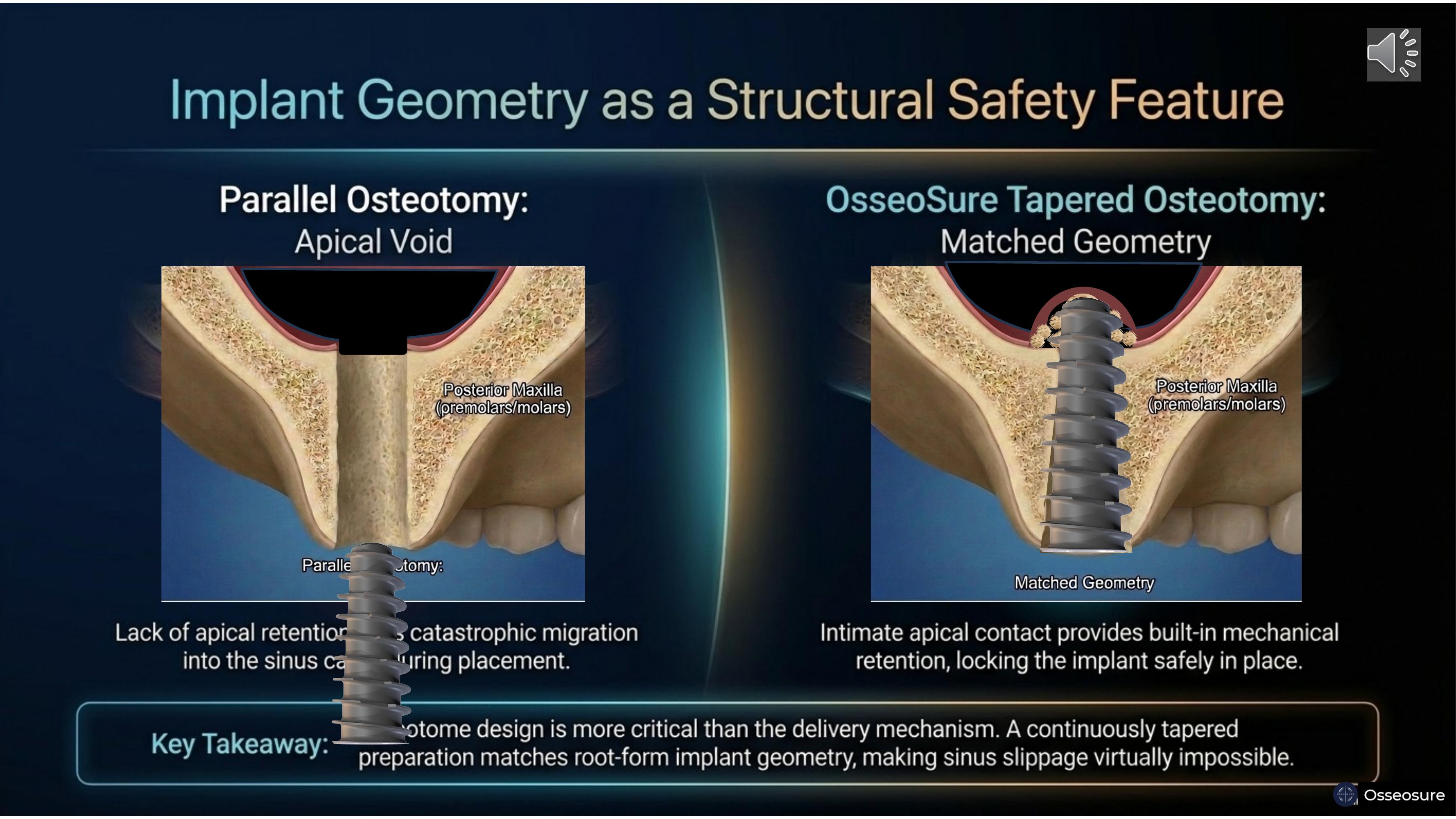
On the left — a parallel osteotomy creates an apical void. No bone contact at the apex. No retention. During placement near the sinus floor, the implant can migrate catastrophically into the sinus cavity.
On the right — OsseoSure's tapered osteotomy matches the root-form implant geometry. Intimate apical contact locks the implant in place. With bicortical fixation. You can see the Schneiderian membrane lifted in a dome shape, the cortical bone fragment still attached to the membrane, and the graft particles beneath. This is the stamp-and-envelope principle in action.
Osteotome design is more critical than the delivery mechanism. A continuously tapered preparation makes sinus slippage virtually impossible.
Slide 17
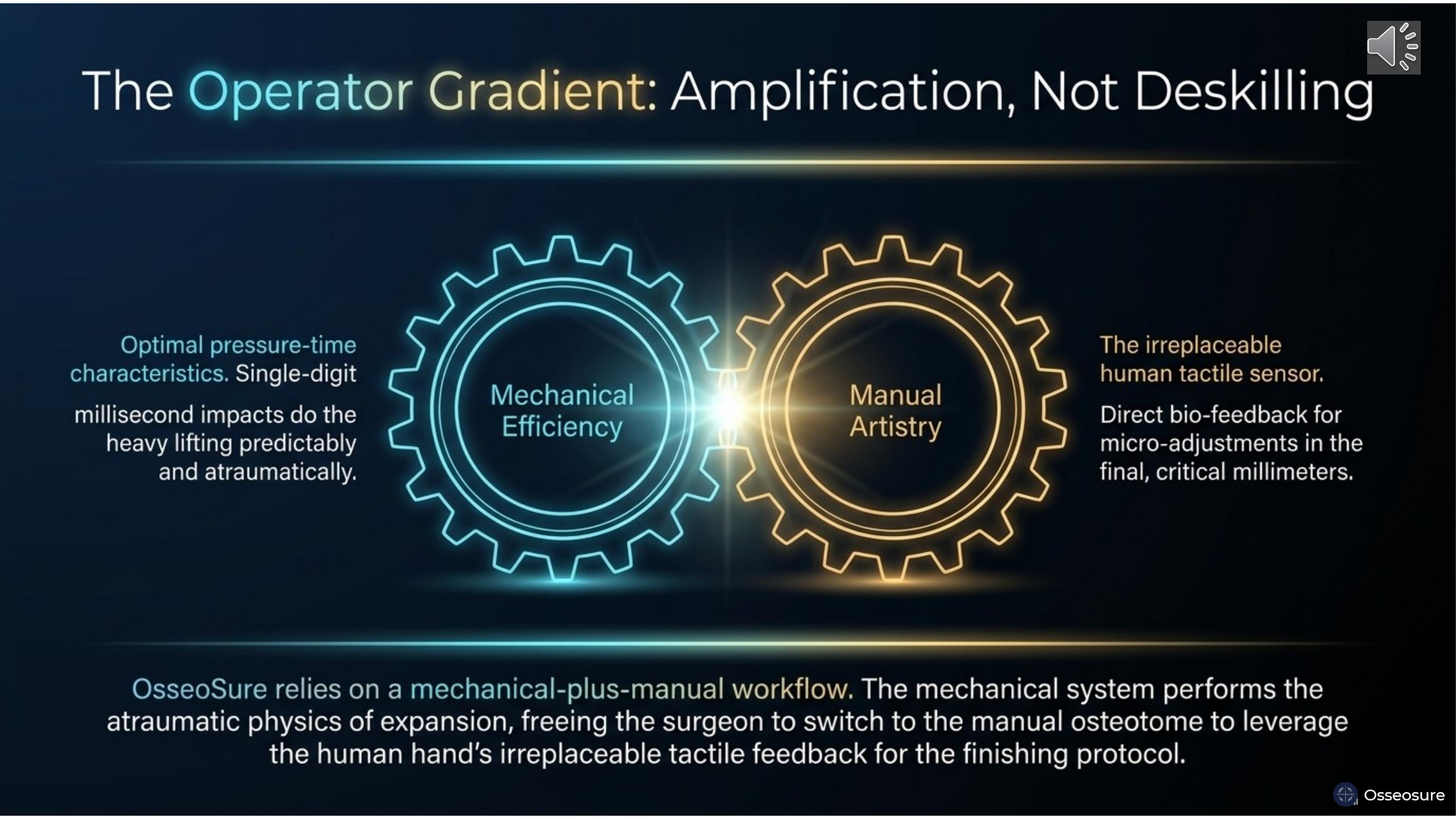
OsseoSure does not replace the surgeon's skill — it amplifies it.
The mechanical system performs the heavy lifting — single-digit millisecond impacts for atraumatic expansion. But the finishing — the final, critical millimeters — requires the irreplaceable human tactile sensor.
OsseoSure relies on a mechanical-plus-manual workflow. Start mechanical or manual. Manual gives trctile sense of bone softness. for the bulk of the preparation use mechanical …….Finish with manual for the refinement. This is amplification, not deskilling.
Slide 18
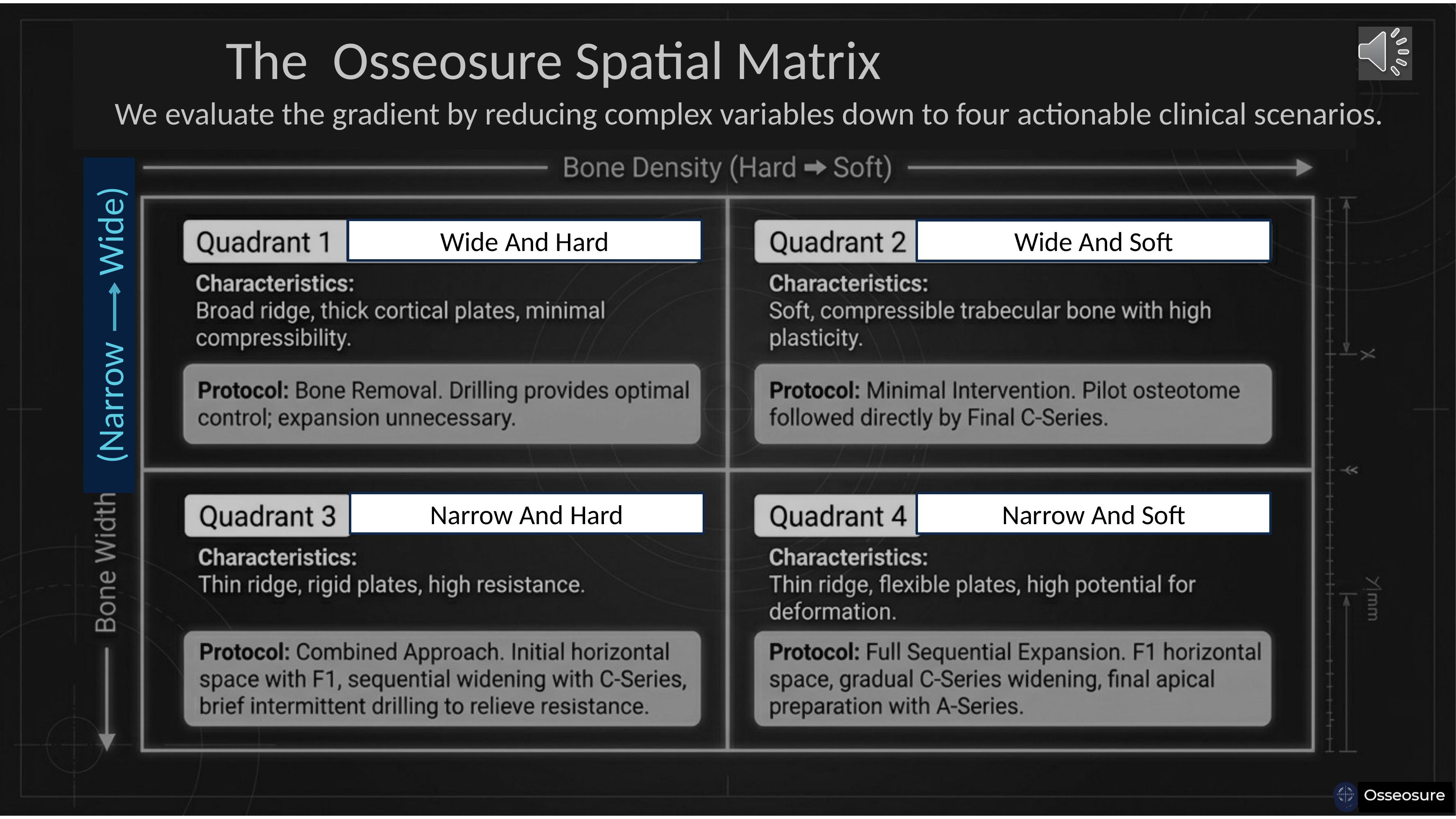
For OsseoSure treatment planning, we consider bone in two dimensions: narrow versus wide, and soft versus hard. From that, we get four quadrants.
Quadrant One — wide and hard bone. Here, you will continue your drilling protocol. There is absolutely no need for OsseoSure.
Quadrant Two — wide and soft bone. Here, you will always think of OsseoSure for bone condensation. You will never use drilling. Pilot osteotome followed directly by the final C-Series.
Quadrant Three — narrow and hard bone. You will first use the F1 tip to create a horizontal split. After that, sequential widening with C-Series osteotomes. At times, you may require partial drilling with a pilot drill to relieve resistance — mostly at the crest or sometimes at the apex.
Quadrant Four — narrow and soft bone. You start with F1 for horizontal splitting, then continue with C-Series. At times, you may require the A-Series for apical preparation. In narrow soft bone, mostly you won't need the A-Series.
This is the simple, clear protocol given by the OsseoSure philosophy.
Slide 19
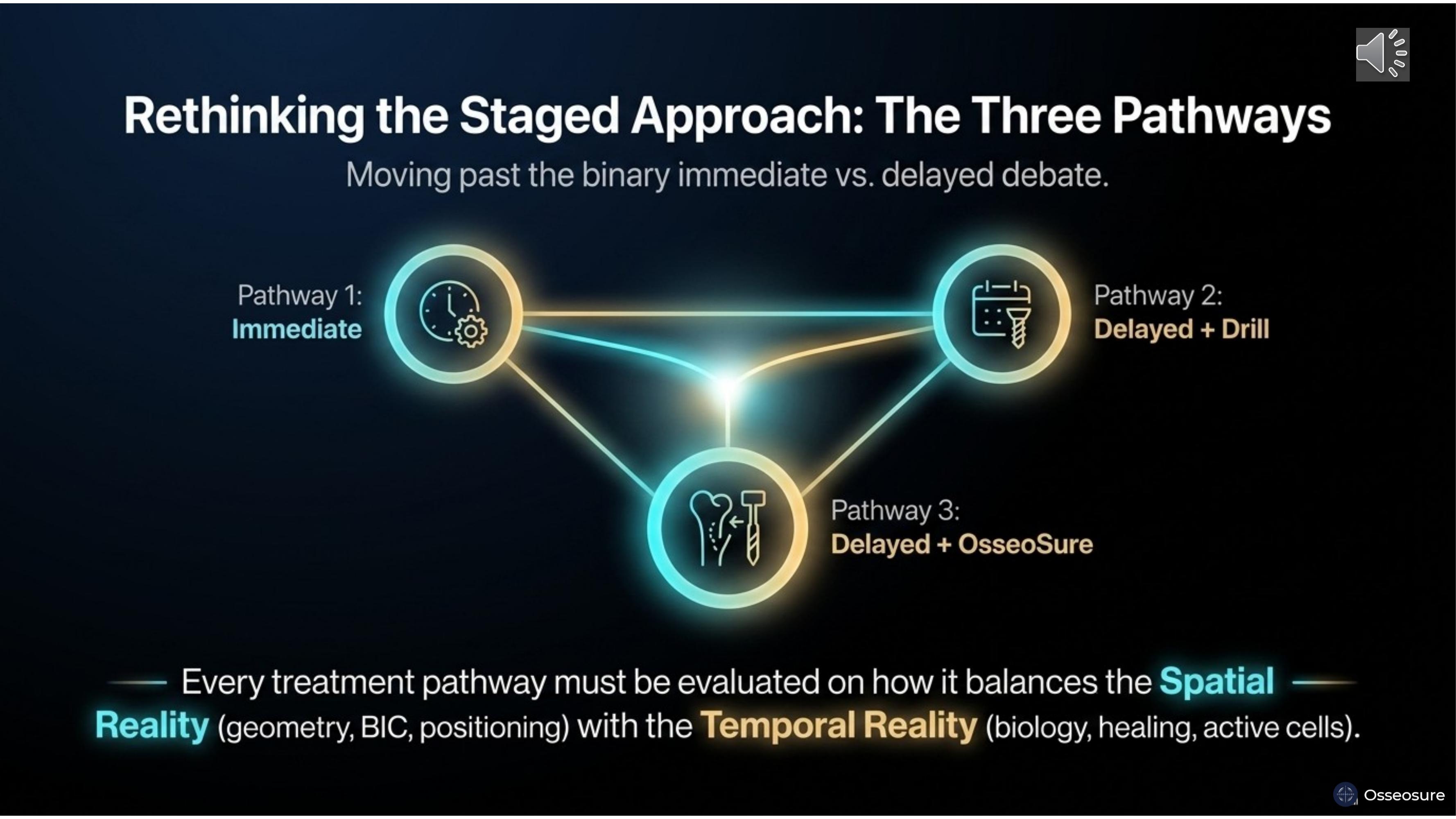
The conventional debate has always been binary — immediate versus delayed. But that is an incomplete question.
There are three pathways. Pathway One: immediate implantation. Pathway Two: delayed placement with conventional drilling. Pathway Three: delayed placement with OsseoSure condensation.
Every pathway must be evaluated on how it balances the spatial reality — geometry, bone-implant contact, positioning — with the temporal reality — biology, healing, cell activation
Slide 20
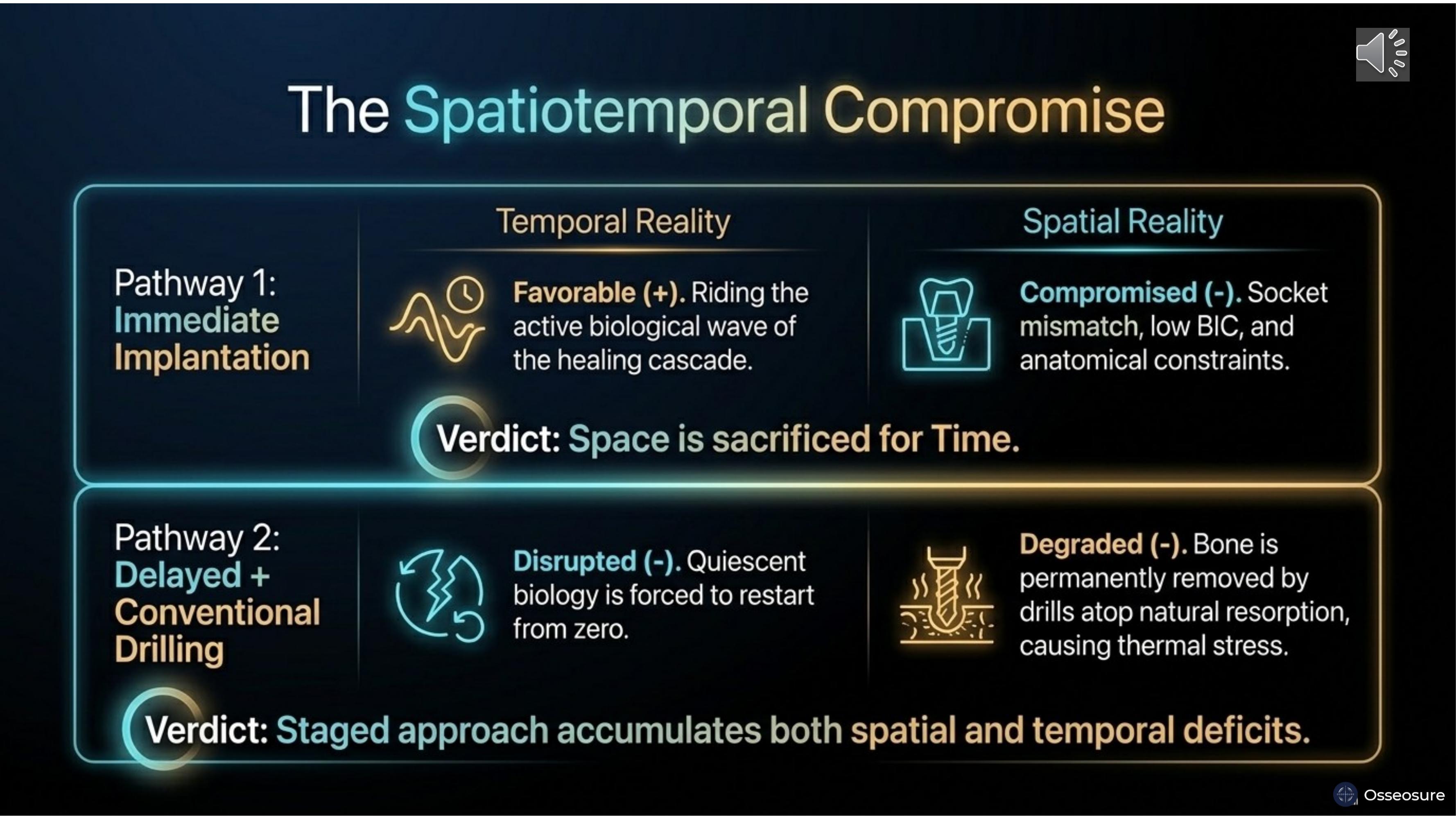
Pathway One — immediate implantation. Temporal reality is favourable — you ride the active healing cascade. But spatial reality is compromised — socket mismatch, low bone-implant contact. Space is sacrificed for time.
Pathway Two — delayed placement with drilling. You wait — the ridge resorbs. Then you drill into already-resorbed bone, removing more volume and creating thermal necrosis. Biology has gone quiescent and it is forced to restart from zero. This staged approach accumulates both spatial and temporal deficits.
Slide 21
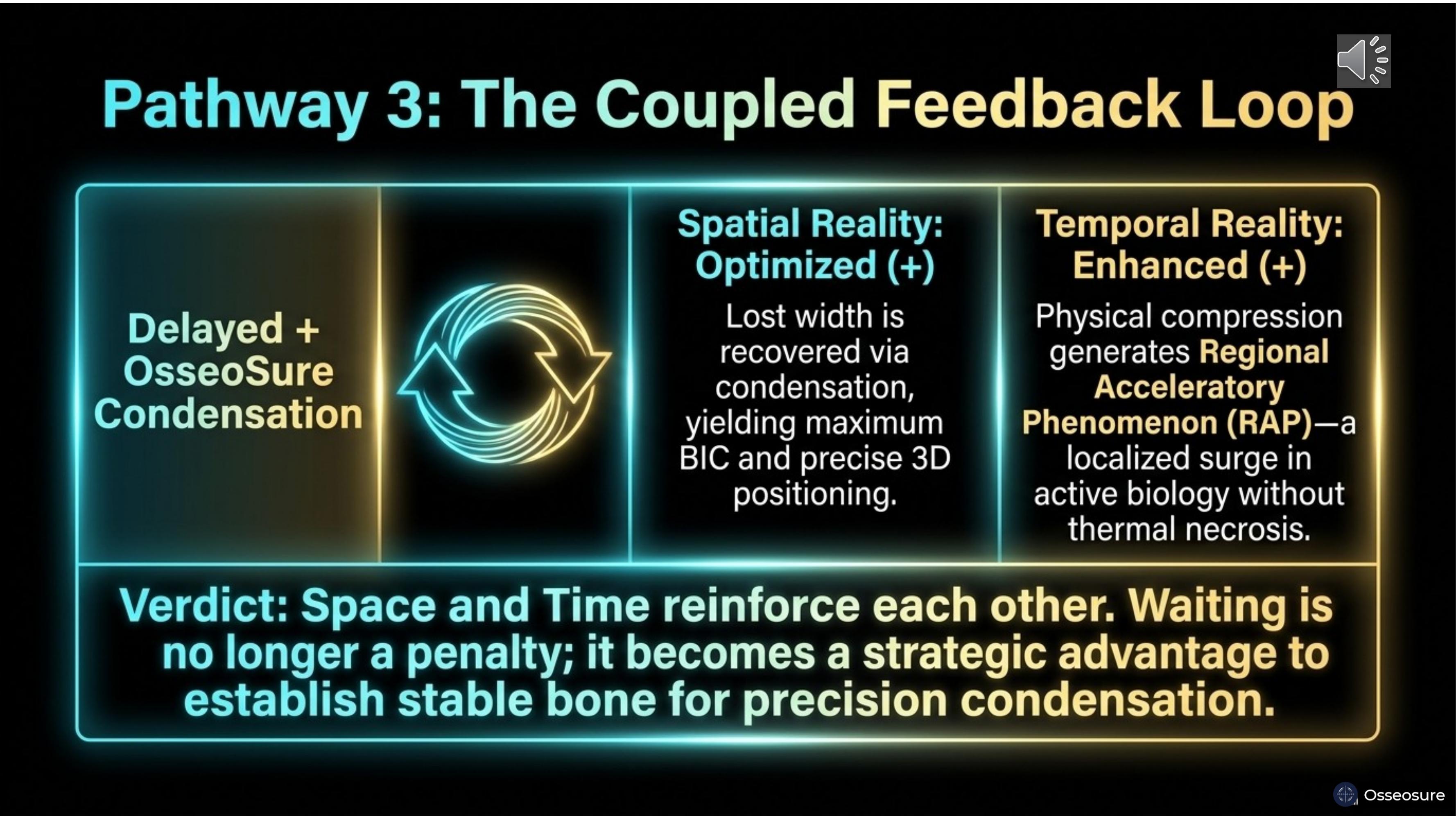
Pathway Three — delayed placement with OsseoSure condensation.
Spatial reality: optimised. Lost width is recovered through condensation. Maximum bone-implant contact. Precise 3D positioning.
Temporal reality: enhanced. Physical compression generates RAP — a localised surge in active biology without thermal necrosis. The healing clock accelerates.
Space and time reinforce each other. Waiting is no longer a penalty — it becomes a strategic advantage. You allow the ridge to stabilise, then use condensation to recover width and simultaneously trigger accelerated healing. This is the coupled feedback loop.
Slide 22
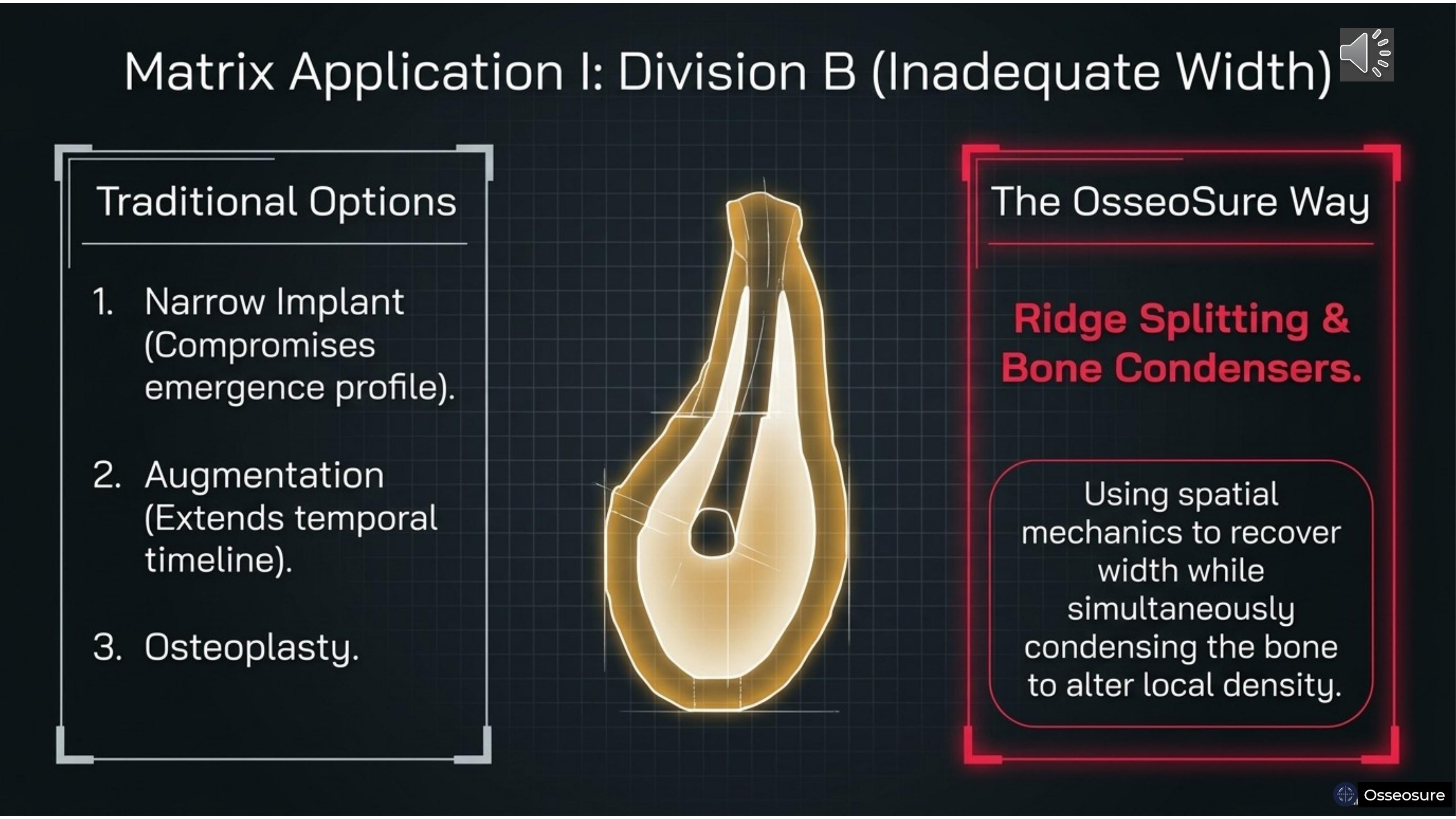
Let us apply the matrix. Division B bone — inadequate width.
Traditional options: a narrow implant — which compromises emergence profile. Augmentation — which extends the temporal timeline by months. Or osteoplasty — which removes even more precious bone. With taller crown.
The OsseoSure Way: ridge splitting and bone condensation. Using spatial mechanics to recover width while simultaneously condensing the bone to improve local density. You solve the spatial problem and gain a temporal advantage in one procedure.
Slide 23
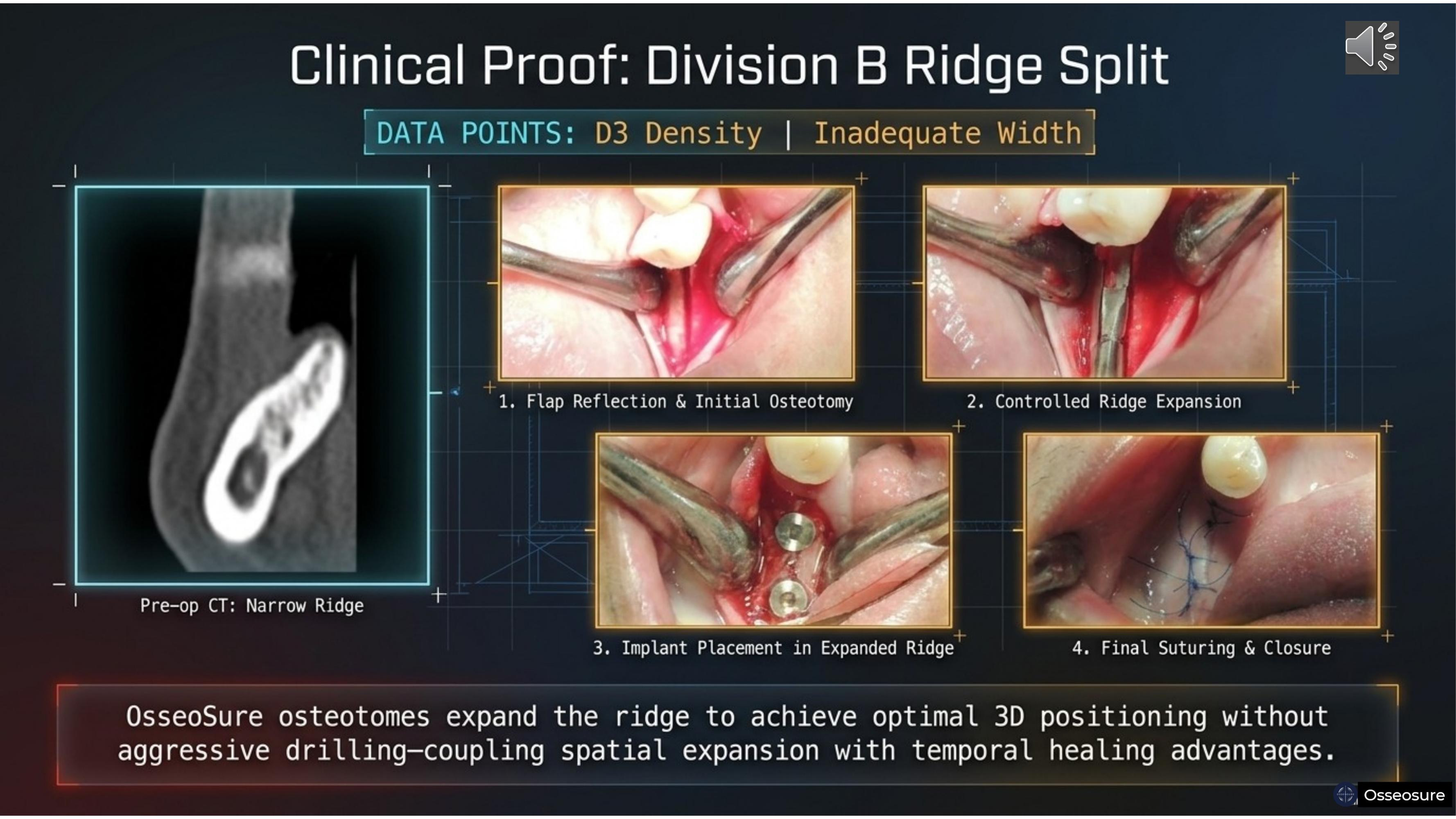
Here is the clinical proof. D3 density, inadequate width. Pre-operative CbcT shows a narrow ridge.
Step one — flap reflection and initial osteotomy with the F1 tip. Step two — controlled ridge expansion with C-Series osteotomes. Step three — implant placement in the expanded ridge. Step four — final suturing and closure.
OsseoSure osteotomes expanded this ridge to achieve optimal 3D positioning without aggressive drilling — coupling spatial expansion with temporal healing advantages.
Slide 24
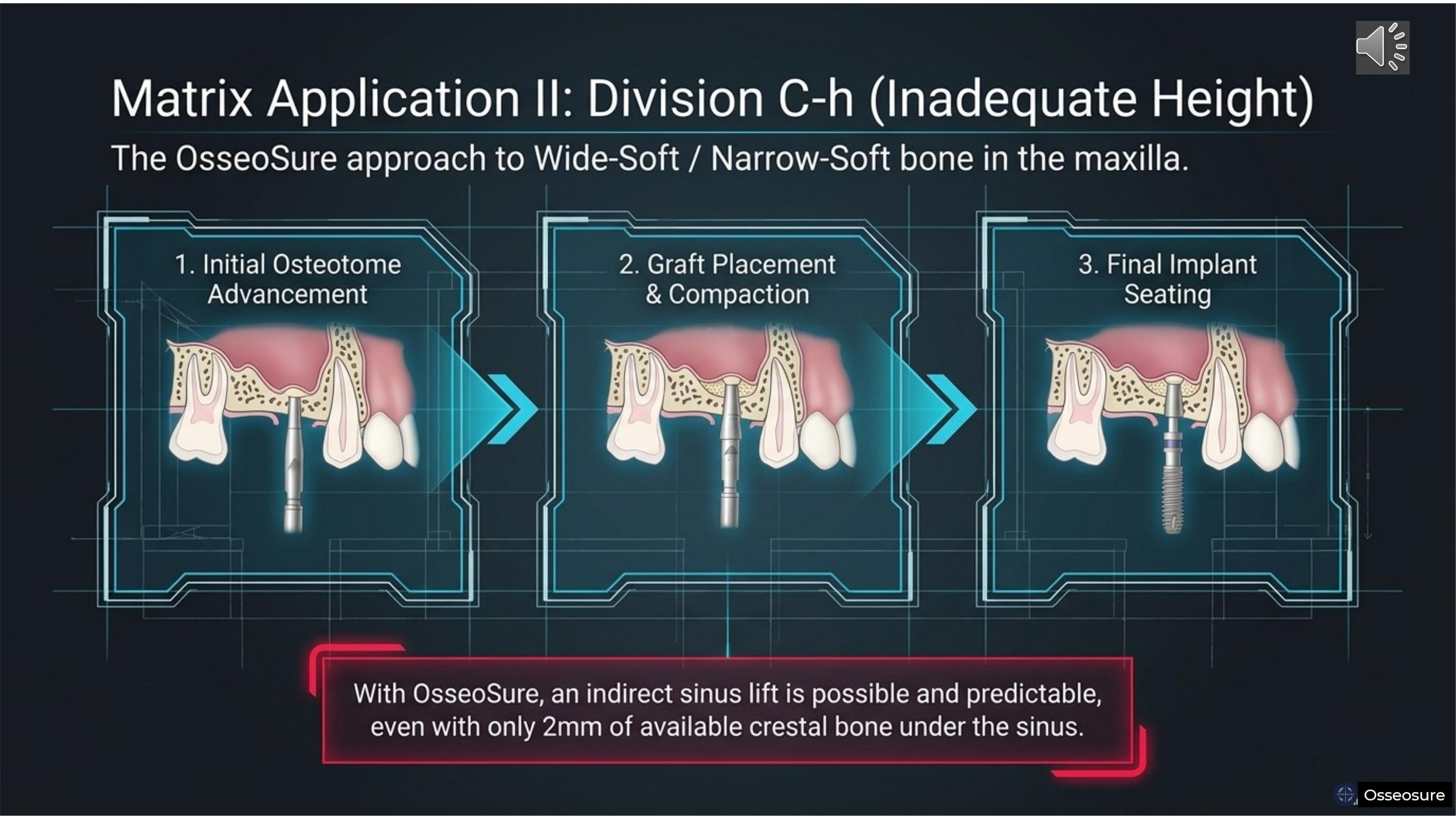
Division C-h — inadequate height. Wide-soft or narrow-soft bone in the maxilla.
With OsseoSure, an indirect sinus lift is possible and predictable — even with only two millimeters of available crestal bone under the sinus. Step one — initial osteotome advancement with p2 and CF Series. Step two — graft placement and compaction beneath the elevated membrane. Step three — final implant seating.
In most cases, one or at most two osteotome tips complete the entire indirect sinus lift. The chances of Schneiderian membrane tearing are virtually eliminated.
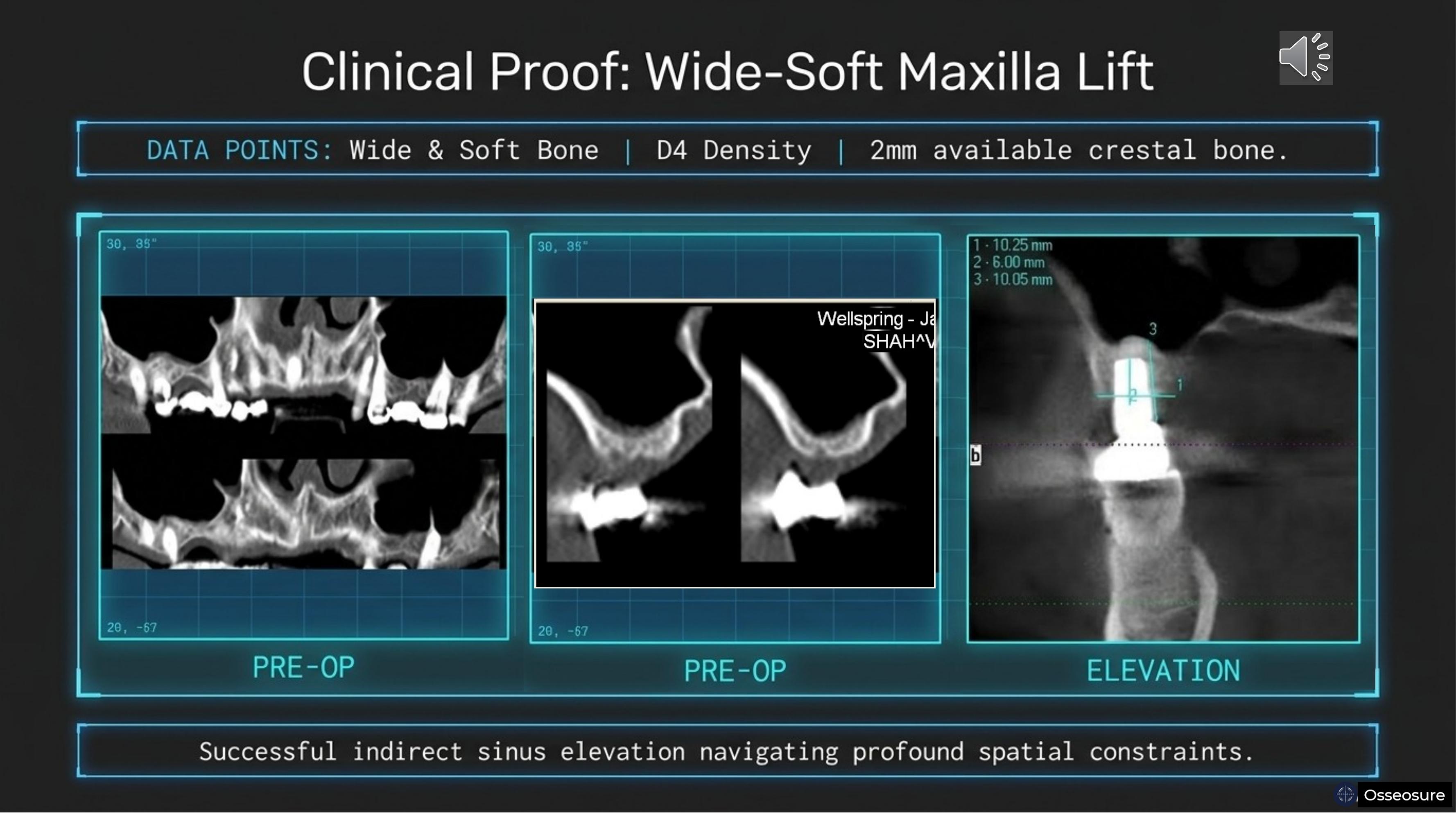
Slide 25
Clinical proof. Wide and soft bone, D4 density, only two millimeters of available crestal bone. Pre-operative imaging on the left. The elevation with OsseoSure in the centre. Post-operative result on the right.
Successful indirect sinus elevation navigating profound spatial constraints — without a lateral wall approach, without membrane perforation, and with the implant in the correct 3D position.
Slide 26
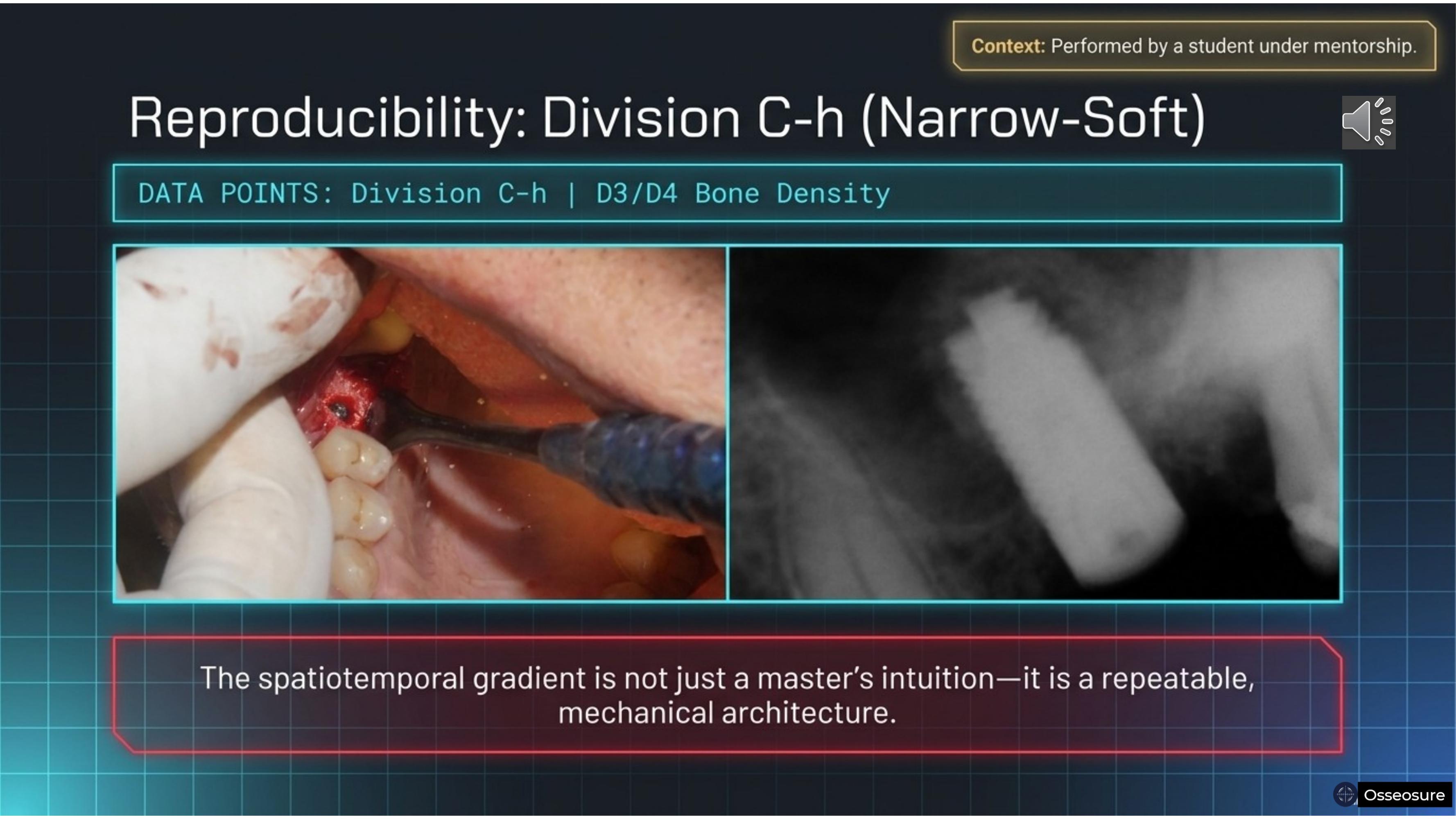
And here is what matters most — reproducibility. This case was performed by my student, under my guidance. Division C-h, D3/D4 bone density.
The spatiotemporal gradient is not just a master's intuition — it is a repeatable, mechanical architecture. When the instrument embodies the physics, the learning curve shortens dramatically. my students have achieve what took me years to master.
Slide 27
Here is the aesthetic proof. On the left — conventional drilling. Implant more buccaly placed .,and result is , the gingival margin recedes. And taller crown
On the right — OsseoSure condensation. Crestal bone is preserved, compacted, densified. The gingival margin is supported. Soft tissue stability is the direct surface expression of crestal bone preservation.
Late implantation cases prepared with OsseoSure can rival or exceed the aesthetic outcomes of immediate placement. That is the power of the coupled feedback loop.
Slide 28
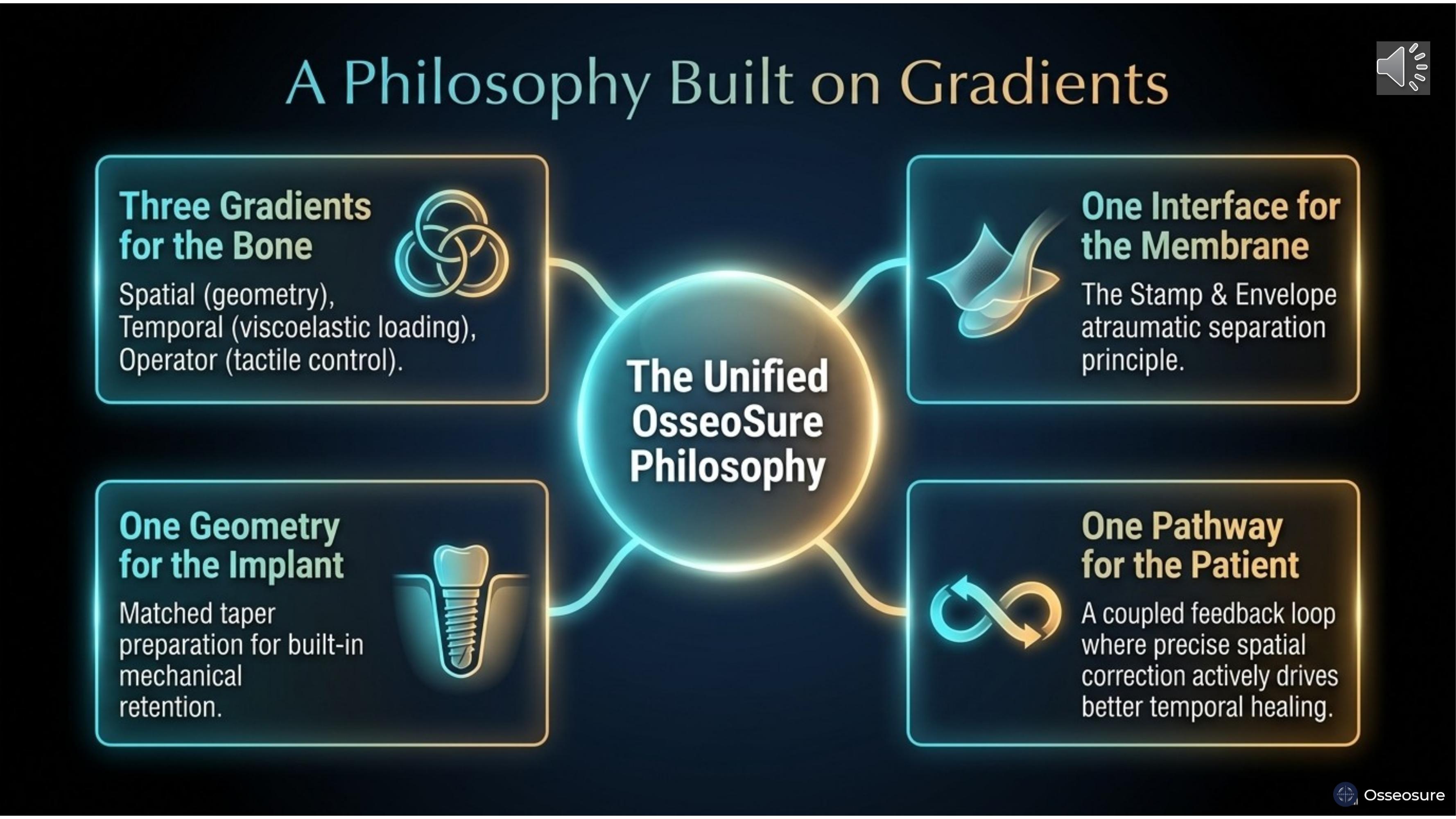
The unified OsseoSure philosophy.
Three gradients for the bone — spatial geometry, temporal viscoelastic loading, and operator tactile control.
One interface for the membrane — the Stamp and Envelope atraumatic separation principle.
One geometry for the implant — matched taper preparation for built-in mechanical retention.
One pathway for the patient — a coupled feedback loop where precise spatial correction actively drives better temporal healing.
Spatial is where. Temporal is when. Spatiotemporal is where and when, together, as one continuous gradient.
Slide 29
You no longer have to choose between spatial compromise and temporal delay.
The OsseoSure way uses space to buy time — and time to build space.
Precision meets trust.
Thank you.
Join the OsseoSure Clinical Community
Free — get notified when new lectures and cases are published.