OsseoSure Clinical Masterclass
The OsseoSure Catalogue
Complete System Overview
19 slides · Speaker: Dr. Kedar Bakshi
Slide Gallery



Slide 3
Every implant dentist faces three pain points in daily practice.
The first pain point is atraumatic extraction. It is very challenging to extract a badly broken-down, root-canal-treated tooth — especially when it is broken at bone level. Extracting without destroying the buccal bone becomes a real challenge.
The second pain point is the sinus. When available bone under the sinus is five millimeters or less, a lateral wall approach becomes necessary for most dentists. And this approach is not easy for everyone to take.
The third pain point is ridge width. After extraction, if the available bone in width is five millimeters or less, it becomes equally challenging.
OsseoSure helps in all three of these pain points. That is its foundation — biological respect, minimal trauma, and maximum predictability.
Slide 4
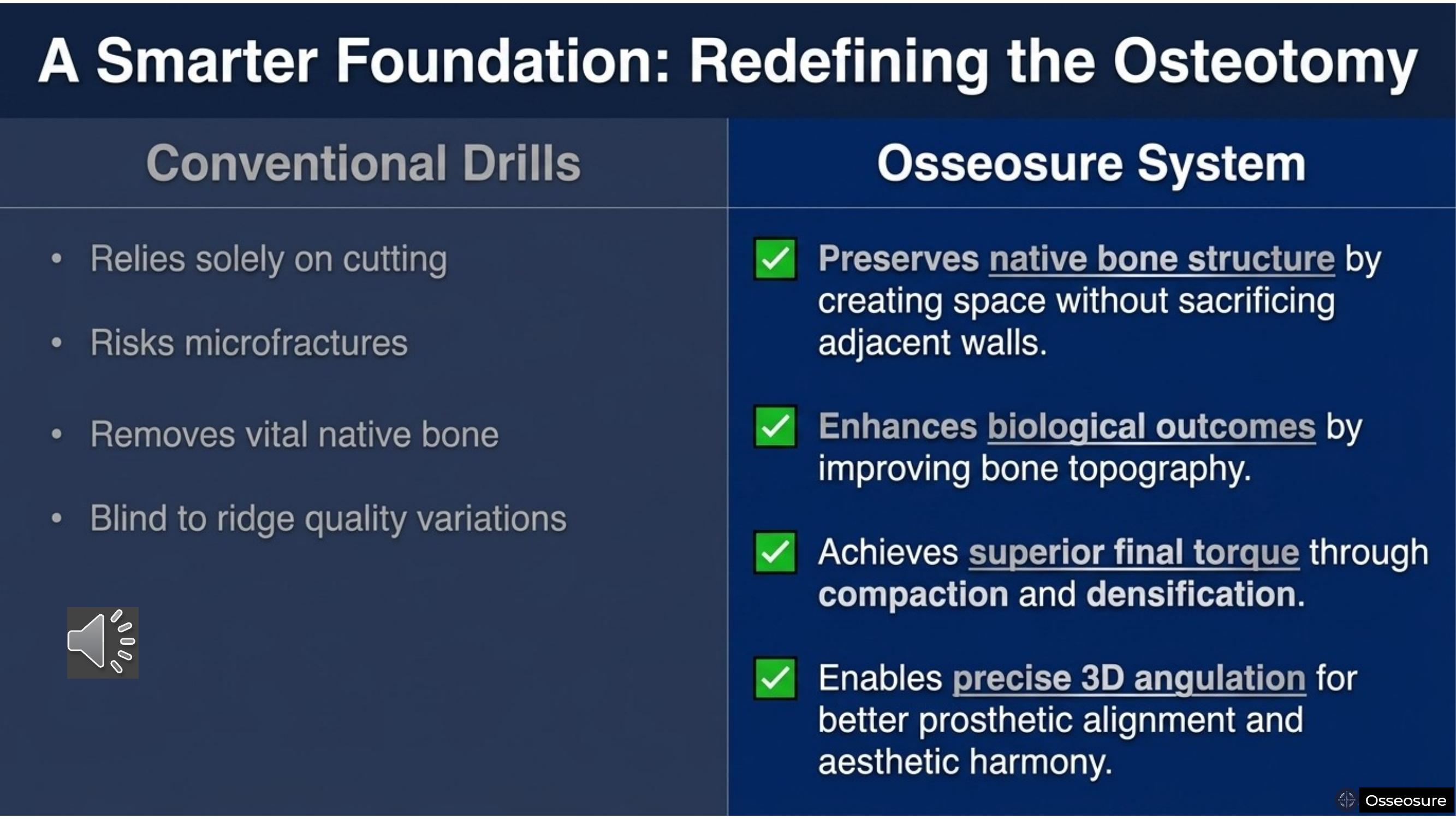
Why are we drilling bone? We are drilling bone because manufacturers have not given us any other option. But now, that option is available — in the form of OsseoSure.
OsseoSure will condense the bone. It will compact the bone. It will enlarge narrow ridges. At the same time, it can help you elevate the sinus floor indirectly — even when the available bone under the sinus is two millimeters or less.
You will always get superior final torque. And you can place the implant with better angulation for aesthetics. In three-dimensional implant positioning, if your angulation is toward the incisal edge or cingulum position, you will always achieve better aesthetics. For that, correct angulation is required — and with the OsseoSure system, you can achieve it. Drilling alone will never allow you to correct the angulation.
Slide 5
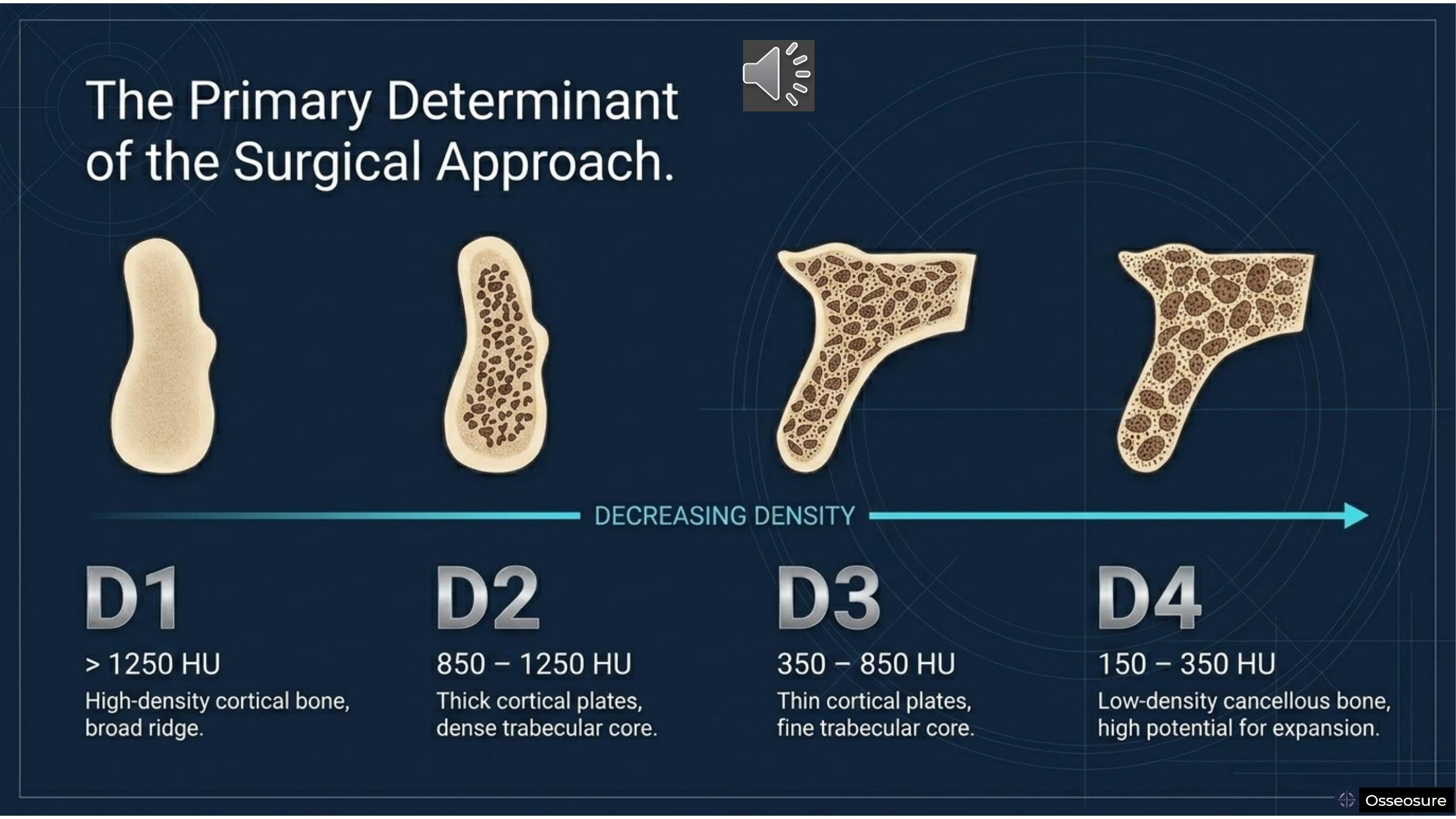
Let's come to treatment planning. Treatment planning is influenced by the available bone — both in quality and quantity.
If bone is D1, D2, D3, or D4 — that is, from hard to soft — this is one way of classifying the bone for quality. D1 is high-density cortical bone with a broad ridge. D2 has thick cortical plates with a dense trabecular core. D3 has thin cortical plates with a fine trabecular core. And D4 is low-density cancellous bone — with high potential for expansion.
Dense compacta
Dense compacta coarse trabeculae
Porus compacta fine trabculae
Slide 6
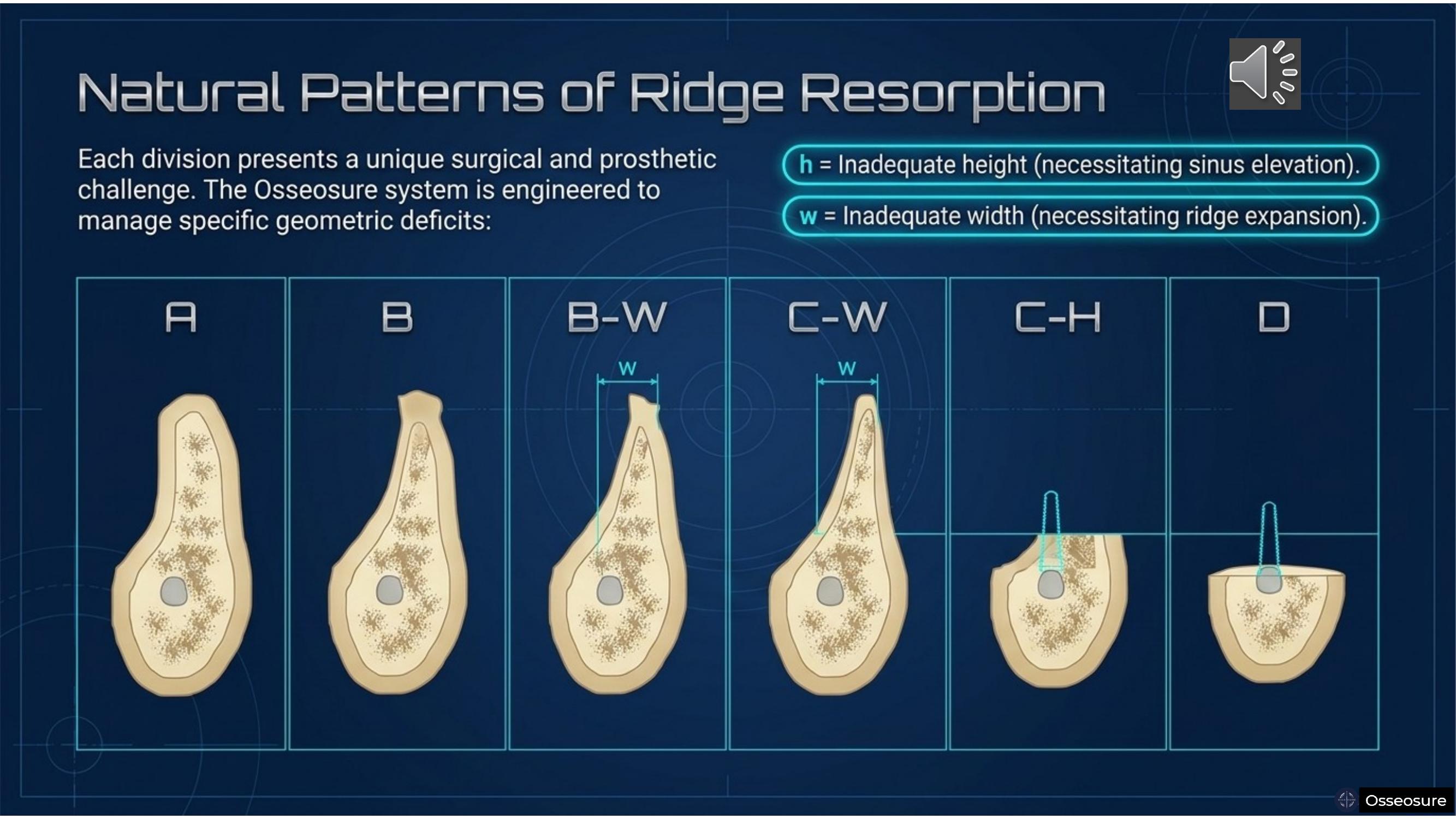
For the quantity of bone, I use the classification which gives us Division A, B, B-W, C-W, C-H, and D. Divisions B-W, C-W, and C-H are very challenging — and this is where the OsseoSure system will help you.
In Division B and B-W, OsseoSure helps with ridge splitting. In C-H, it helps with indirect sinus elevation. And if Division A bone is soft, it helps with bone condensation.
Slide 7
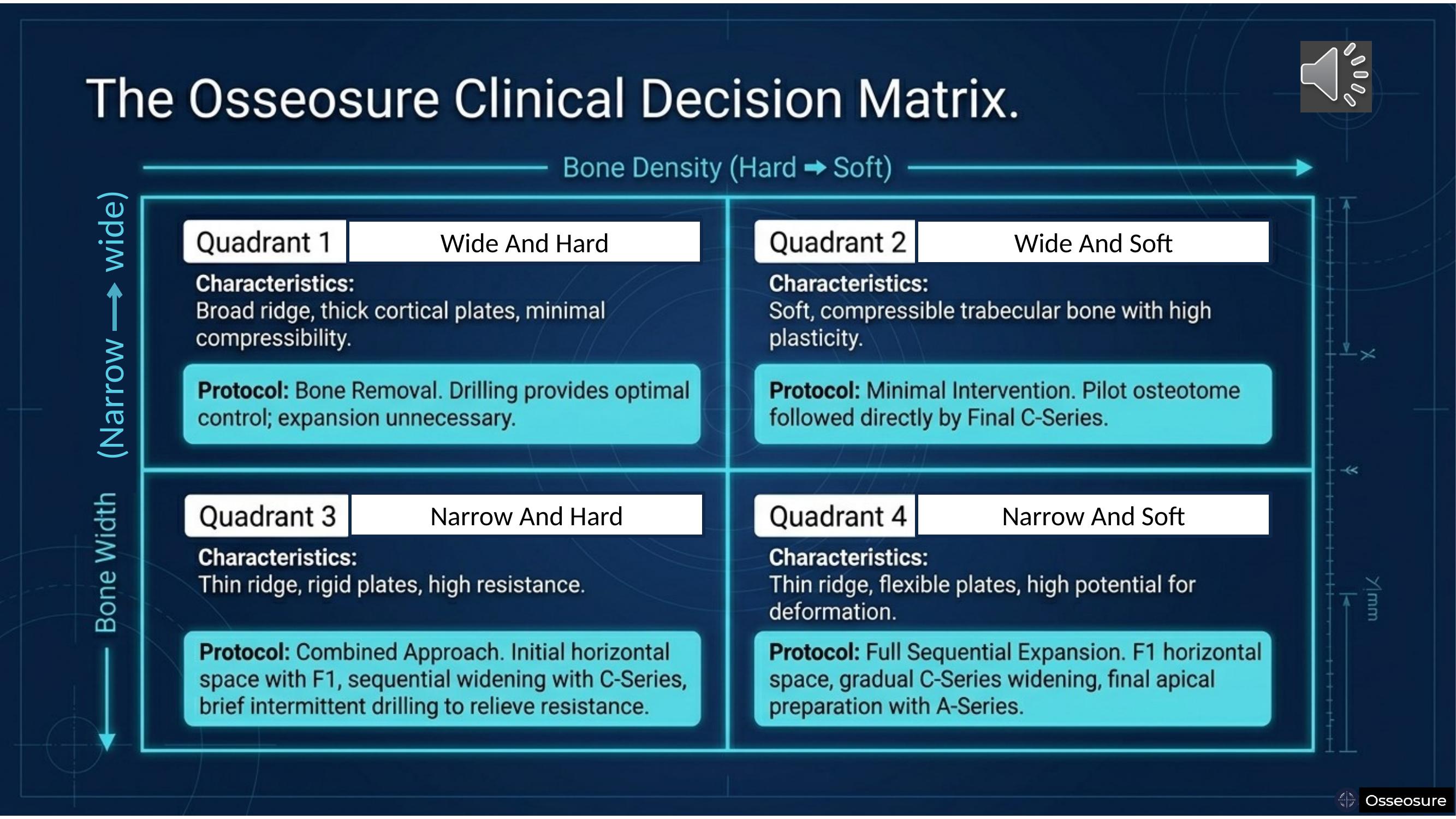
For OsseoSure treatment planning, we consider bone in two dimensions: narrow versus wide, and soft versus hard. From that, we get four quadrants.
Quadrant One — wide and hard bone. Here, you will continue your drilling protocol. There is absolutely no need for OsseoSure.
Quadrant Two — wide and soft bone. Here, you will always think of OsseoSure for bone condensation. You will never use drilling. Pilot osteotome followed directly by the final C-Series.
Quadrant Three — narrow and hard bone. You will first use the F1 tip to create a horizontal split. After that, sequential widening with C-Series osteotomes. At times, you may require partial drilling with a pilot drill to relieve resistance — mostly at the crest or sometimes at the apex.
Quadrant Four — narrow and soft bone. You start with F1 for horizontal splitting, then continue with C-Series. At times, you may require the A-Series for apical preparation. In narrow soft bone, mostly you won't need the A-Series.
This is the simple, clear protocol given by the OsseoSure philosophy.
Slide 8
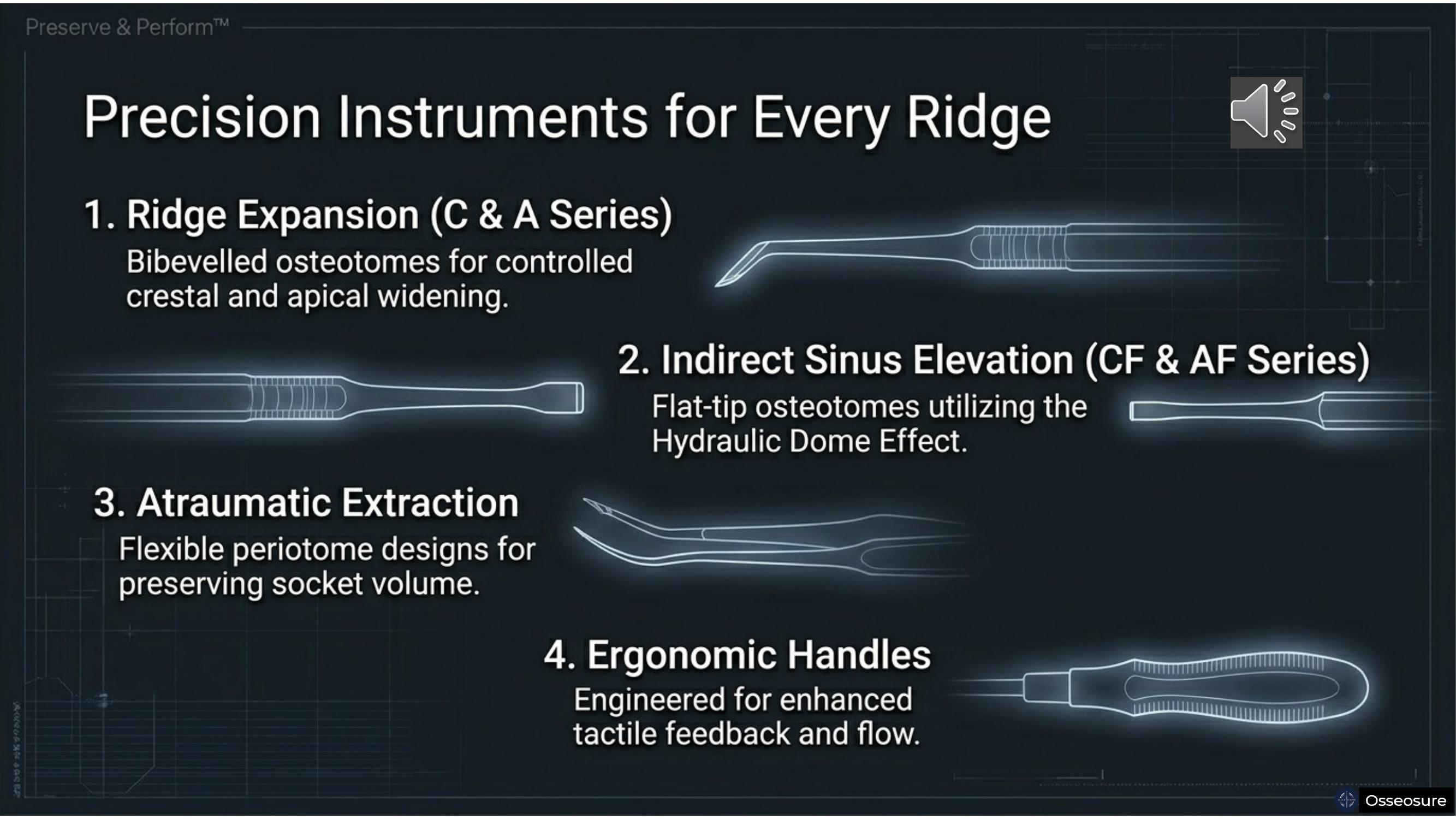
OsseoSure covers four domains — ridge expansion, atraumatic extraction, indirect sinus elevation, and ergonomic handling.
We do not claim that only mechanical osteotomes are superior. At times, manual osteotomes are required — because manual osteotomes give the tactile feedback to the dentist that the mechanical osteotome cannot provide. Your finesse will come from manual osteotomes.
We always recommend a combined effort — mechanical and manual. Initially, you start with mechanical osteotomes. You do most of the work mechanically. And the finishing — the refinement — you do with manual osteotomes.
Slide 9
In the OsseoSure system, we have P1 and P2 — the pilot osteotomes. The apical diameter of P1 is 0.5 millimeters. The apical diameter of P2 is 1.5 millimeters. Both have a taper length of eight millimeters, and 2.2 millimeter of diameter.
P1 is used mostly in harder bone. P2 is used in softer bone. In hard bone, you may use P1 first, then P2 sequentially. In soft bone, after P2, you can directly progress to C 3.6 or C 4.0 osteotomes.
---
Slide 10
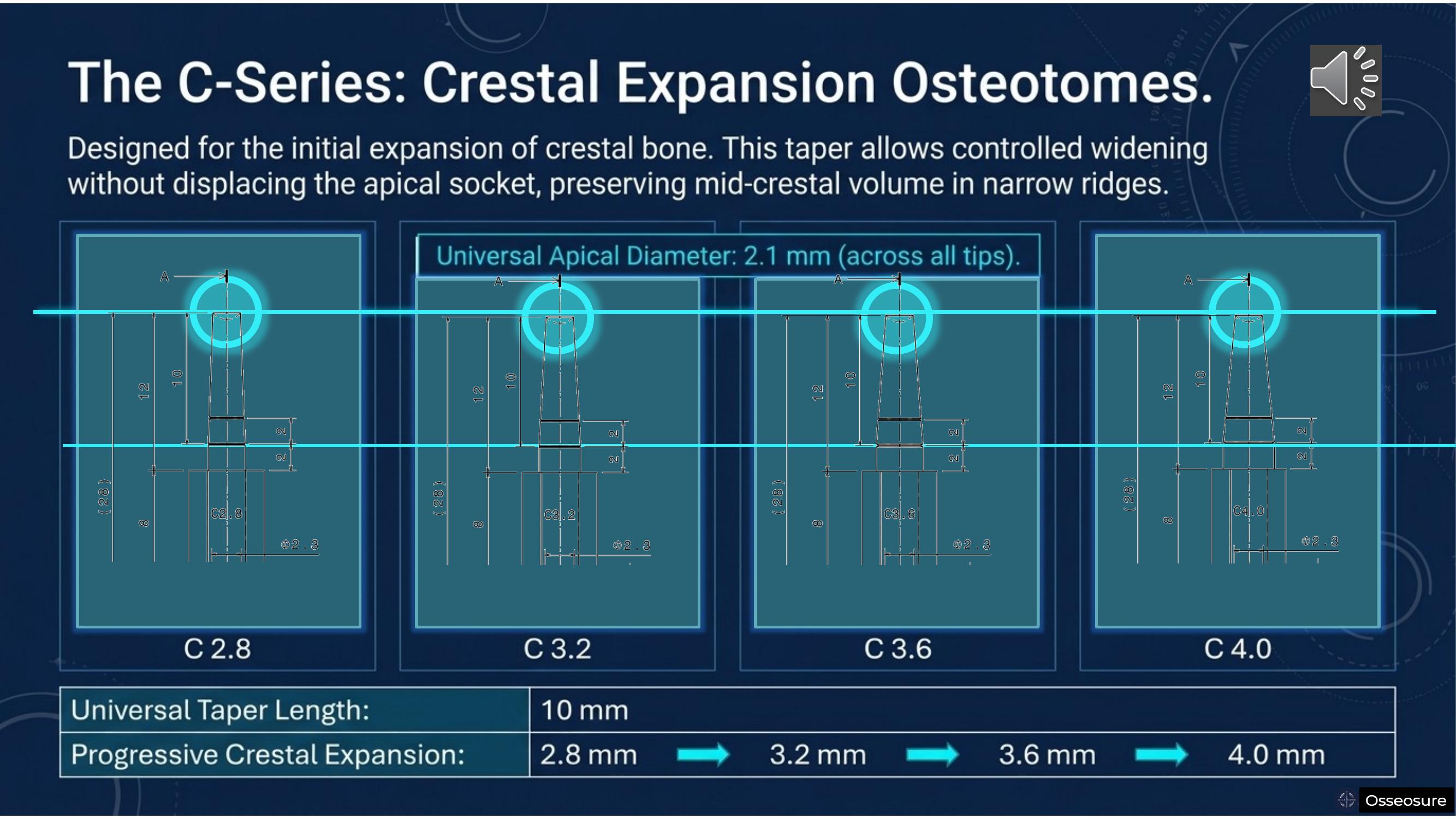
The unique feature of the C-Series is that all tips share a universal apical diameter of 2.1 millimeters. That means C 2.8, C 3.2, C 3.6, and C 4.0 — all of them — enter the osteotomy at the same 2.1-millimeter apical point. Their taper length is ten millimeters, and the crestal expansion progresses from 2.8 to 3.2 to 3.6 to 4.0 millimeters.
This is the crestal expansion phase — controlled widening of crest is achieved
Slide 11
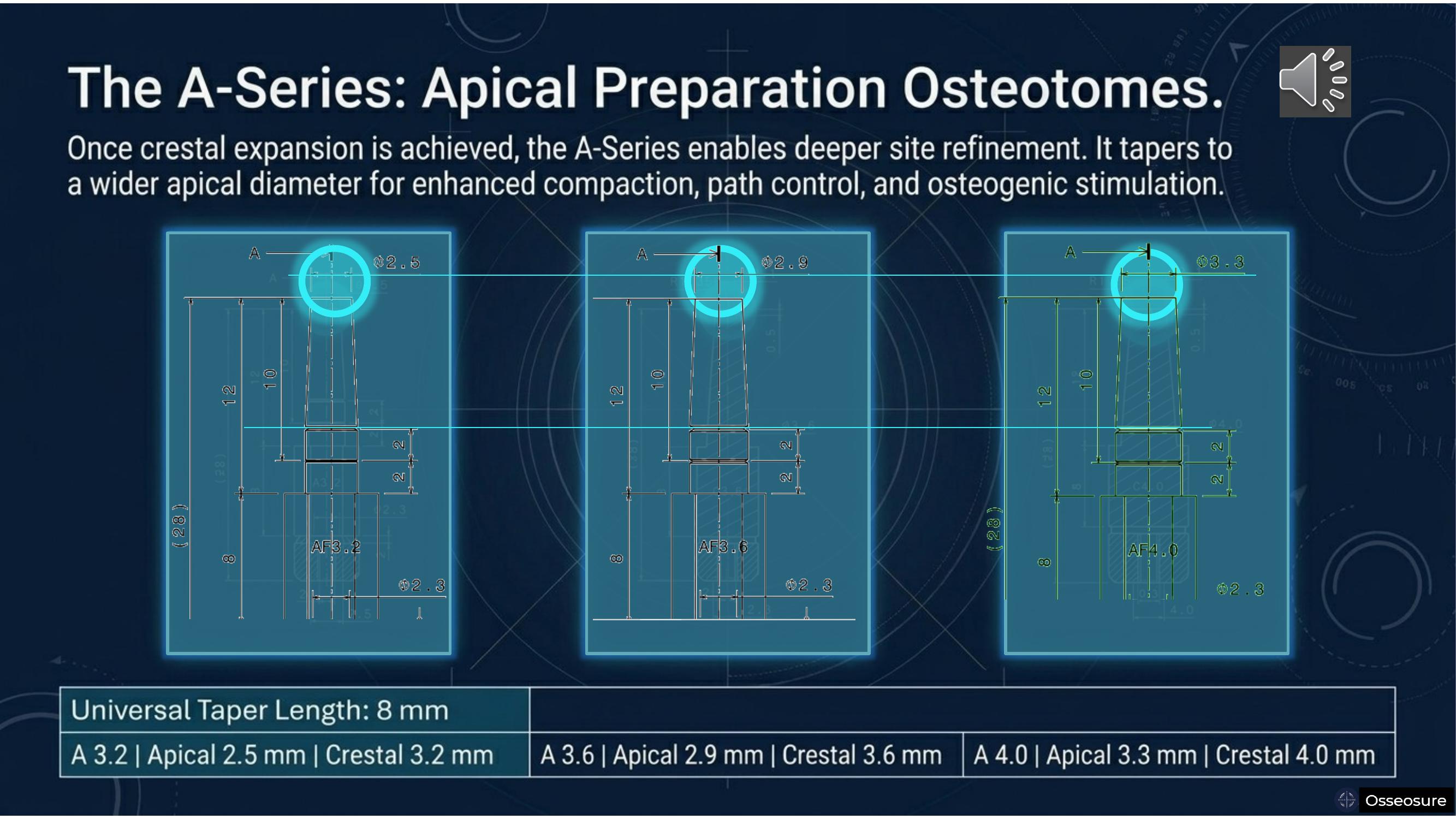
After crestal bone preparation, you can think of preparing the apical bone. Normally, when we drill an osteotomy in hard bone, there is always the possibility that the crestal bone becomes over-enlarged — because resistance at the crest destroys more bone than intended. And if you fail to reach the full depth at the apex, two things happen: either your implant keeps rotating at a certain depth without advancing, or after reaching full depth, you don't have sufficient torque.
This does not happen with OsseoSure — because at any given time, you can prepare bone apically as well. The A-Series osteotomes are designed for this. The system is universal — you can use it for any implant design.
There is a 0.7-millimeter difference between apical and crestal dimensions. For A 3.2, the apical diameter is 2.5 millimeters. For A 3.6, it is 2.9 millimeters. And for A 4.0, it is 3.3 millimeters.
Slide 12
Now you may ask — can I use C-Series tips for indirect sinus? Or can I use CF-Series tips for ridge splitting?
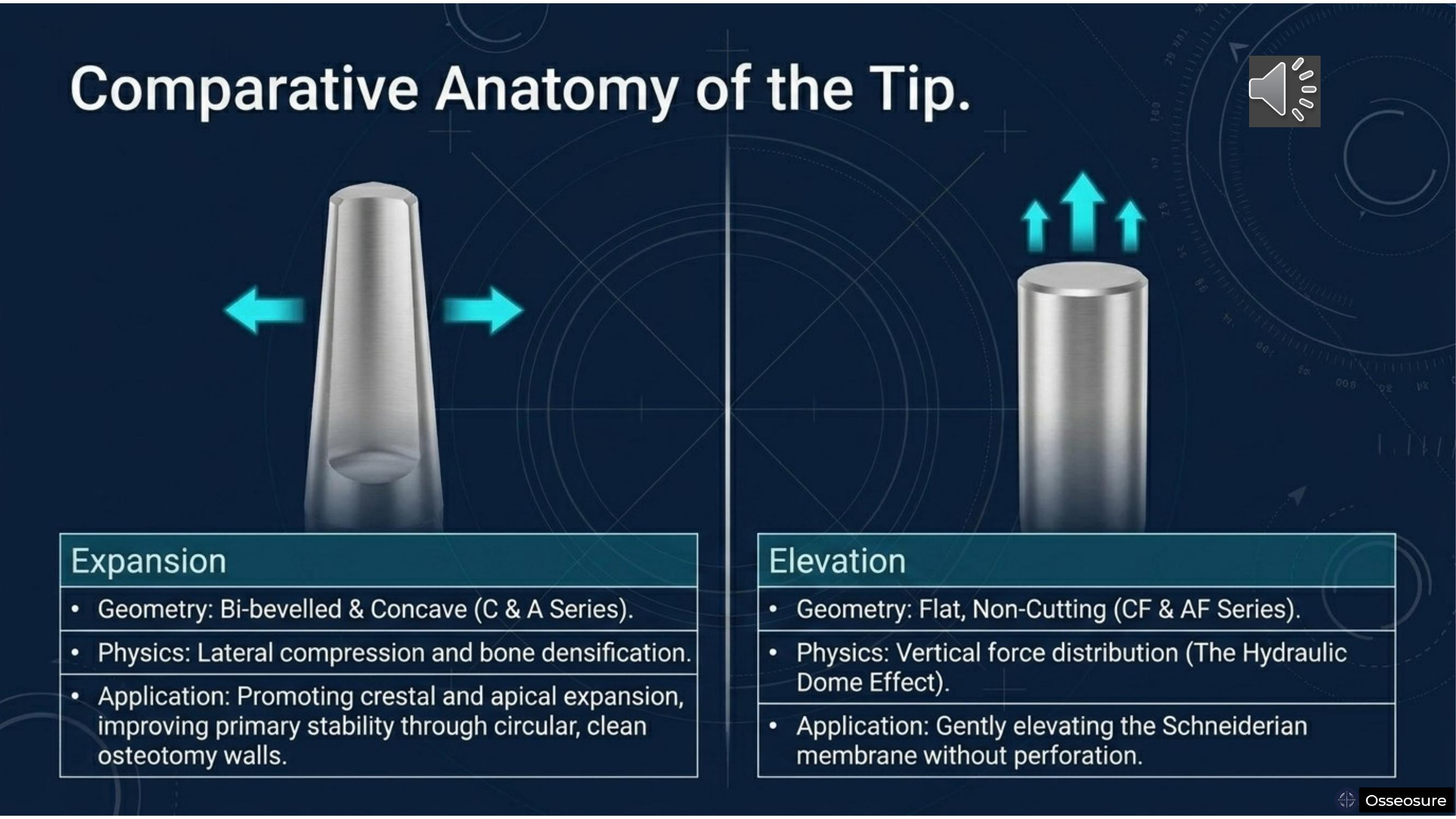
The simple answer is: yes, you can use C and CF Series interchangeably. But it is always advised that you use C-Series for ridge splitting and bone expansion — because the C-Series has a bibevelled concave surface at the apex, designed for lateral compression.
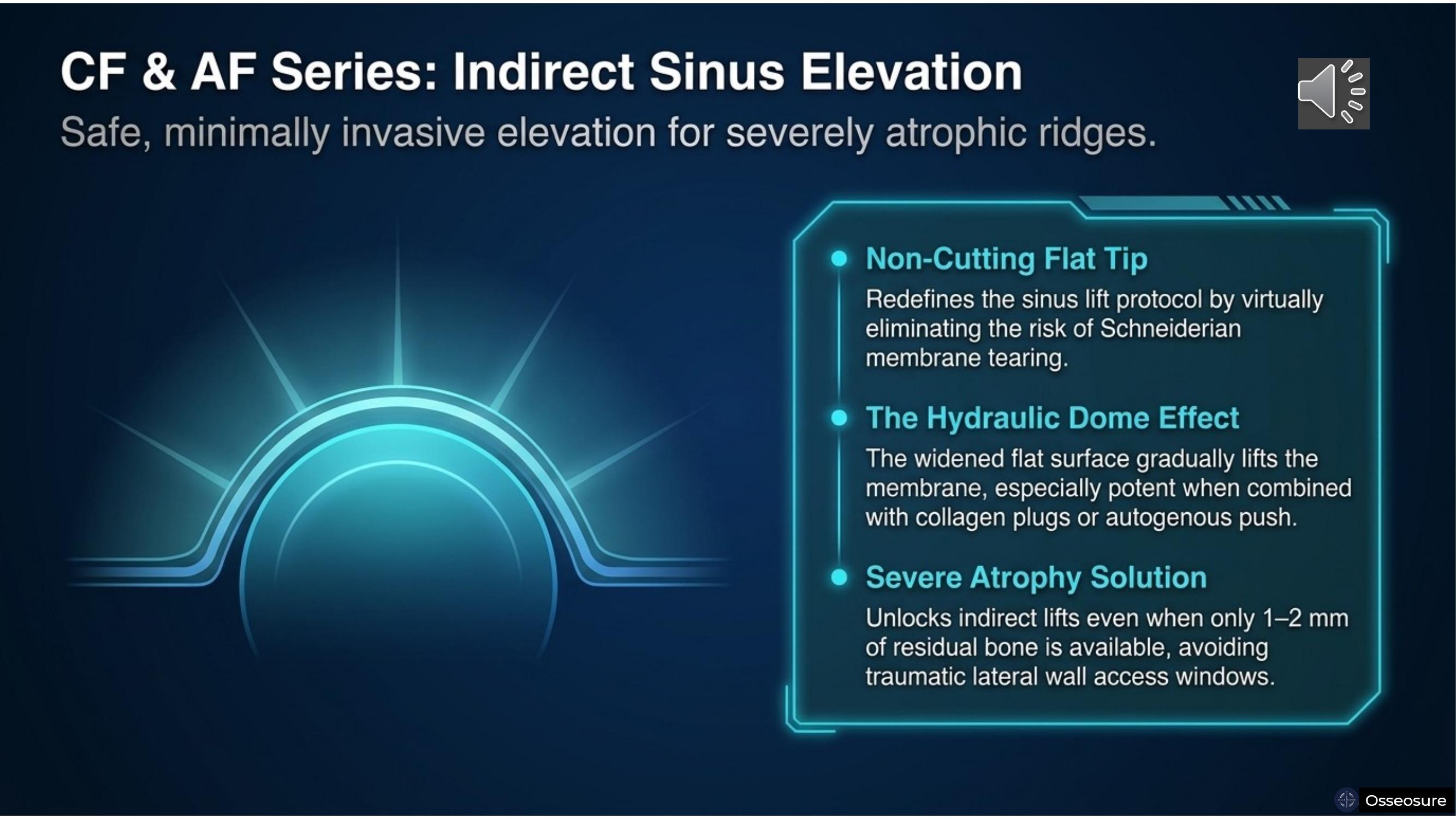
The CF and AF Series have a flat, non-cutting surface — specifically designed to protect the Schneiderian membrane. With a flat tip, membrane perforation becomes virtually impossible.
Slide 13
In indirect sinus cases, the bone is typically having less density — it is softer bone, and the problem is insufficient height. In this scenario, you may initially use a pilot osteotome — perhaps P2, briefly, either manually or mechanically. Then you progress directly to your final osteotome tip — most of the time, CF 4.0.
So in one osteotome tip, or at most two, your indirect sinus lift is complete. The chances of Schneiderian membrane tearing are virtually impossible — if you follow the protocols.
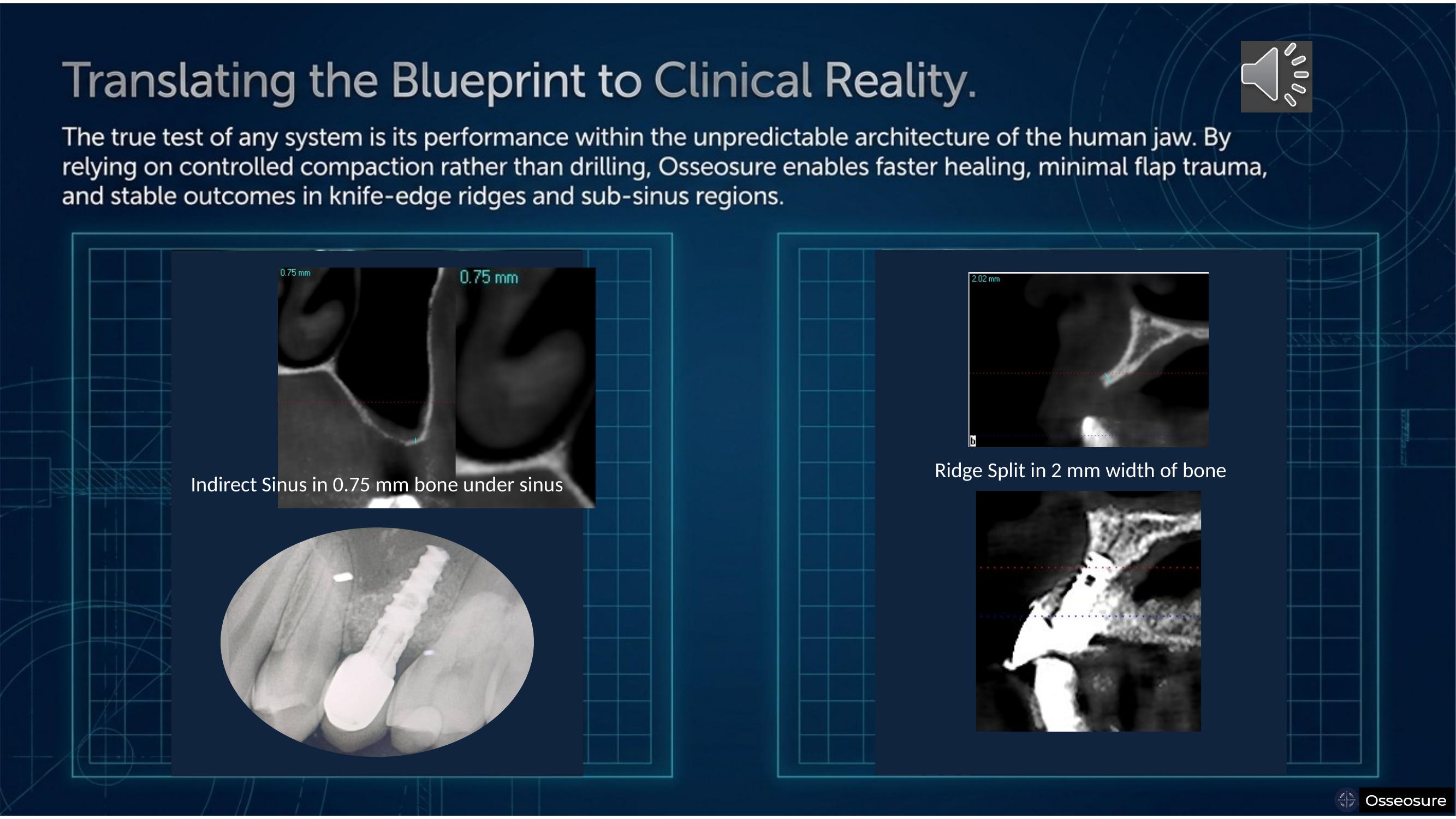
I will show you the case where I have achieved an indirect sinus lift in 0.75 millimeters of available bone. I don't expect everyone to start at 0.75 or one millimeter immediately. But all my students are successfully performing indirect sinus lifts in under two millimeters of available bone. So why not you?
Slide 14
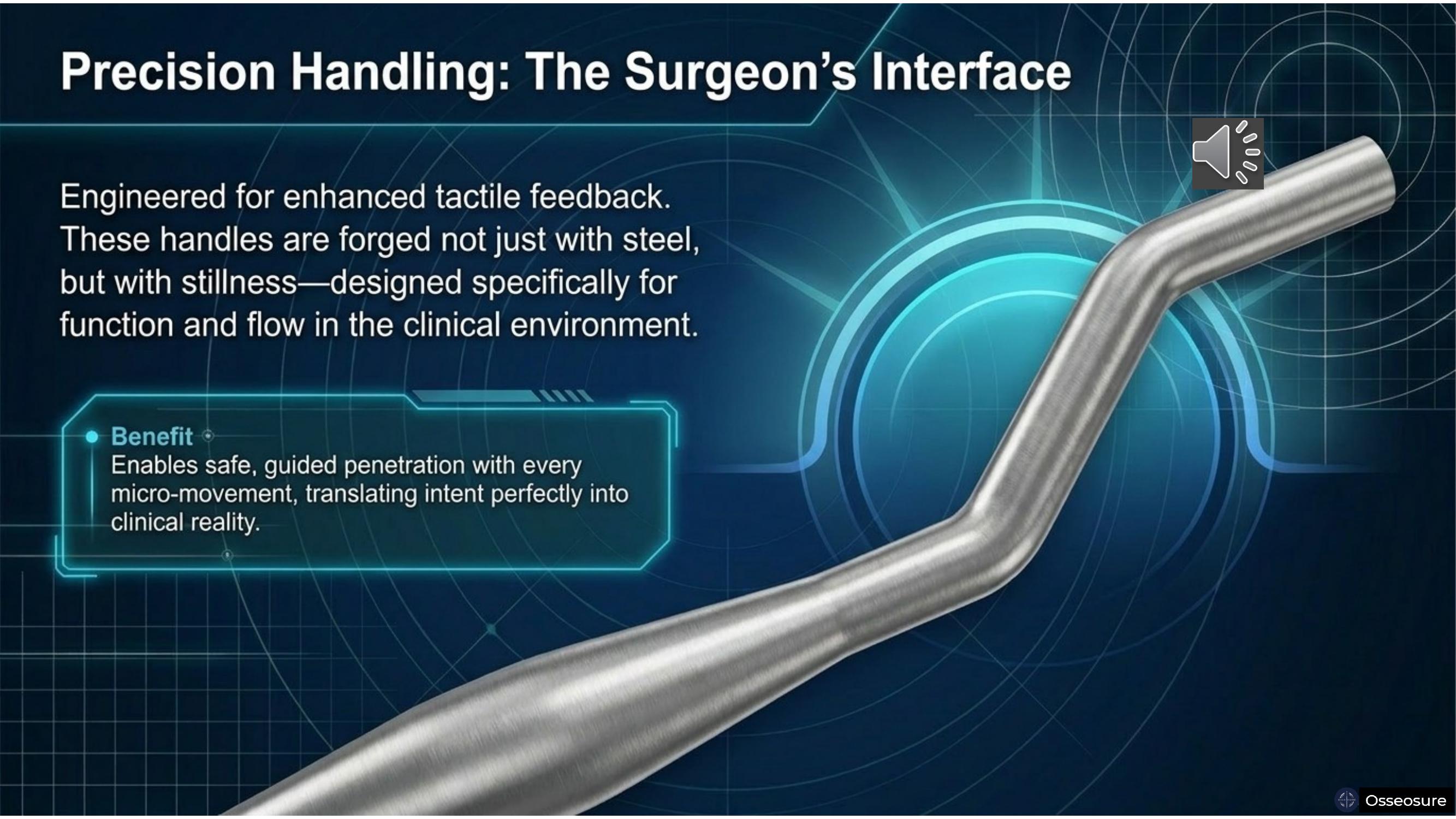
OsseoSure offers three handle configurations — straight, angled, and extra-offset. We do not recommend using extra-offset handles manually — because in manual use, there is less control over the offset geometry.
But extra-offset handles are very effective when used mechanically — particularly in the posterior mandible and posterior maxilla, where access is limited.
These handles are engineered for tactile feedback and clinical flow — forged not just with steel, but with stillness.
Slide 15
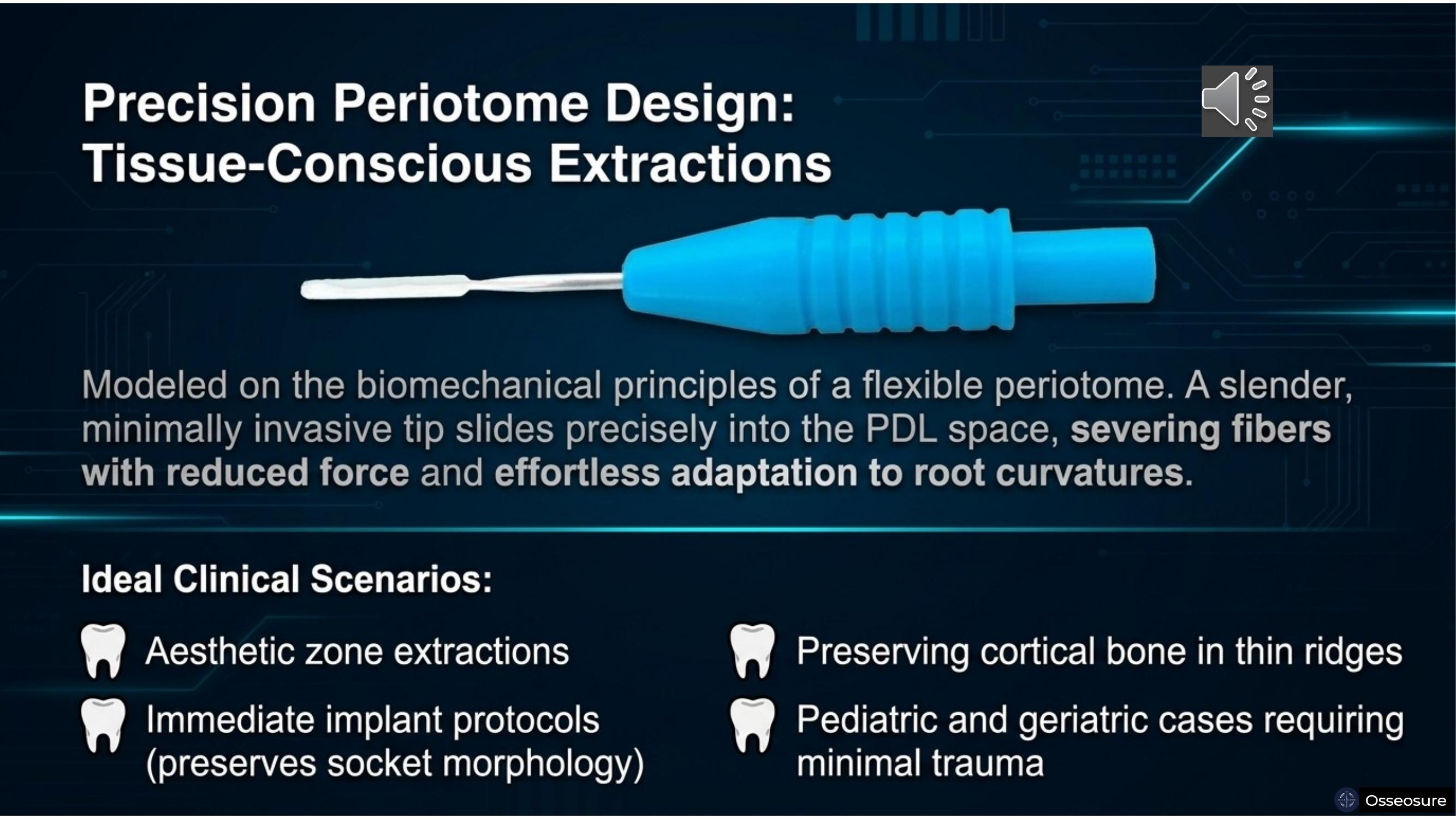
The periotome tips are very thin and flexible — almost fifty microns thin. They slide between the root and the bone, into the periodontal ligament space, and cut the periodontal ligaments very effectively. The tooth loosens, and with any elevator or forceps, it comes out very easily.
This is critically important: if you use a conventional elevator on a root-canal-treated, badly broken-down tooth, the root piece goes on getting crumbled. With OsseoSure periotomes, it will not crumble.
Once you have used the periotome tip, at times you will use the F1 tip to create a little more space. F1 enters the periodontal ligament space already created by the periotome — and with that, your extraction becomes simple and effortless.
Slide 16
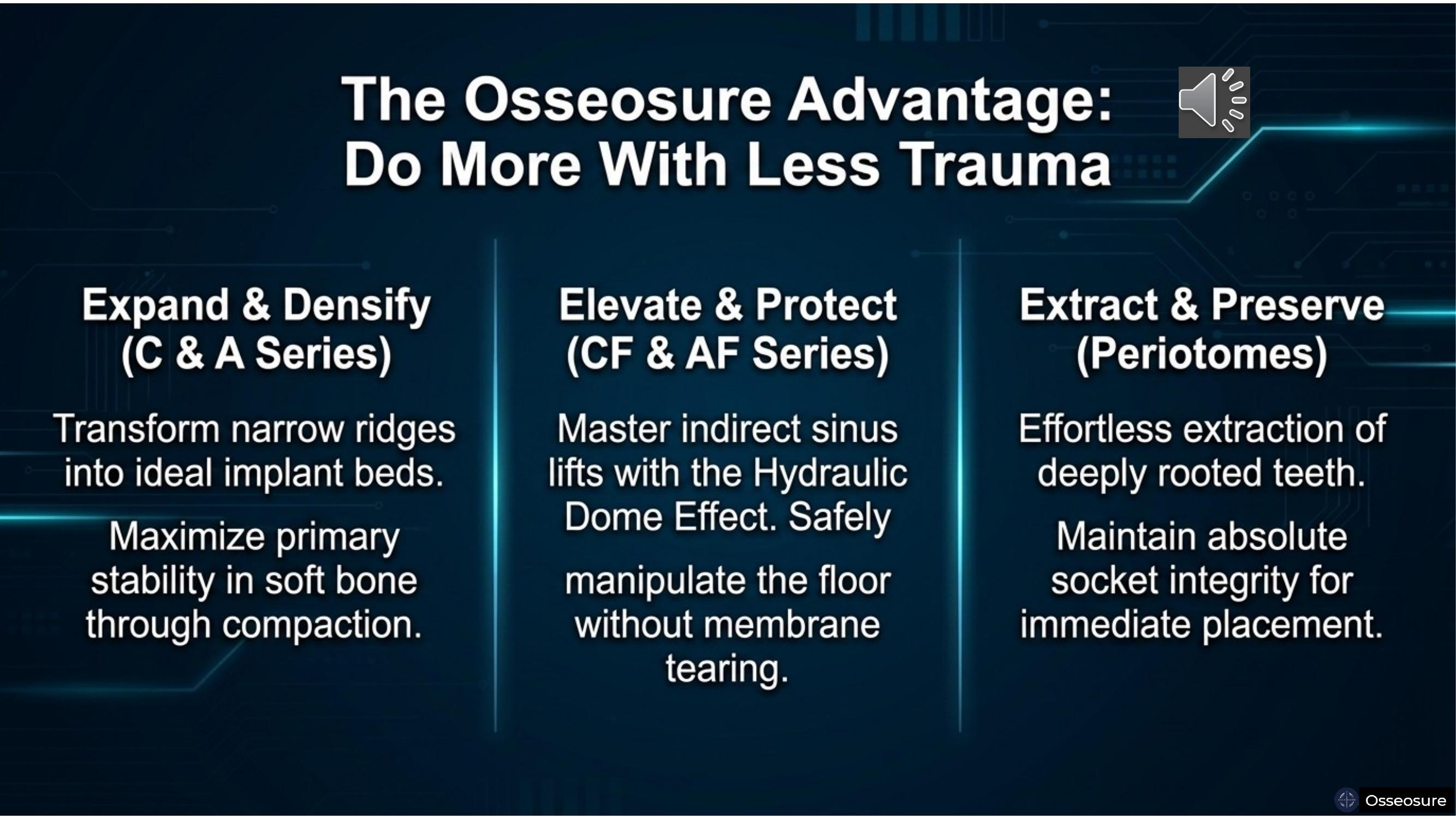
So OsseoSure helps in three ways. It expands and densifies — improving bone density, improving final insertion torque, and improving ISQ values. It elevates and protects — virtually eliminating the need for lateral wall approaches by protecting the Schneiderian membrane during indirect sinus lifts. And it extracts and preserves — enabling successful extractions in all patients, all cases, while preserving the socket for immediate placement.
Your surgeries become more conservative. The healing period is less. And you will not have any performance anxiety — you will always be relaxed and confident.
Slide 17
The true test of any system is its performance within the unpredictable architecture of the human jaw. These are actual CBCT scans — real clinical cases where OsseoSure has been used in knife-edge ridges and sub-sinus regions. By relying on controlled compaction rather than drilling, OsseoSure enables faster healing, minimal flap trauma, and stable long-term outcomes.
Slide 18
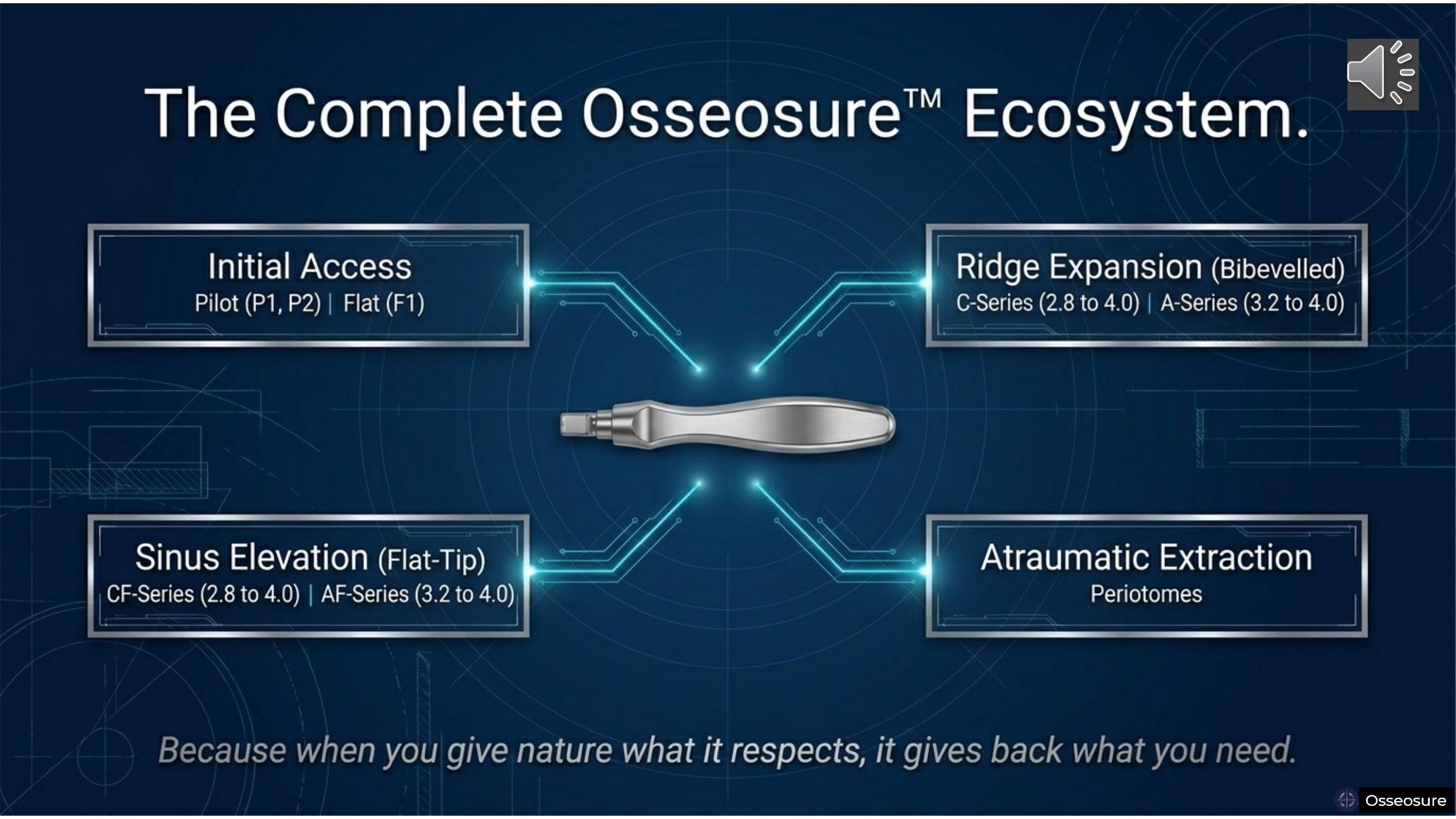
So OsseoSure is your complete ecosystem — initial access with Pilot Series and Flat tips, ridge expansion with C and A Series, sinus elevation with CF and AF Series, and atraumatic extraction with periotomes.
It preserves the bone, and it performs for you.
Because when you give nature what it respects, it gives back what you need.
Slide 19
May your work be peaceful. May your hands be precise. May the lives you touch, transform.
Join the OsseoSure Clinical Community
Free — get notified when new lectures and cases are published.